Points of interest…
- Bowlby identified four sequential stages of attachment development, from indiscriminate sociability at birth through goal-corrected partnership by age three.
- Ainsworth's research produced four recognized attachment styles: secure, anxious-ambivalent, avoidant, and disorganized.
- Only 52% of children worldwide display secure attachment patterns according to cross-cultural meta-analytic research.
- Social workers apply attachment theory across micro, mezzo, and macro practice levels, from individual therapy to child welfare policy design.
Early caregiver bonds shape emotional development and lifelong relationship patterns, a premise that underpins one of the most widely applied frameworks in social work. Attachment theory, developed by John Bowlby in the mid-twentieth century and refined by Mary Ainsworth's classification research, now anchors assessment protocols in child welfare, clinical mental health, and family services alike.
The theory's reach extends from infant observation to adult psychotherapy, and it appears regularly on the ASWB licensing exam. Understanding Bowlby's developmental stages, Ainsworth's attachment styles, validated assessment tools, and documented limitations equips practitioners to translate decades of research into evidence-informed decisions at the case level. For broader context on where attachment theory fits within the field, the social work theories and practice models hub offers a useful starting point.
What Is Attachment Theory?
What does attachment theory actually mean for social work practice, and why do so many assessment frameworks trace back to it?
Attachment theory is a developmental psychology framework that explains how the bonds formed between infants and their primary caregivers shape a person's expectations, emotions, and behaviors in relationships across the entire lifespan. The British psychiatrist and psychoanalyst John Bowlby developed the theory through his clinical work and research from the 1950s through the 1970s, arguing that human infants are biologically wired to seek closeness to a protective adult. Psychologist Mary Ainsworth then gave the theory its empirical footing through her landmark Strange Situation experiments in the 1970s, which identified distinct patterns in how children respond when separated from and reunited with their caregivers.
Three Core Concepts You Need to Know
Grasping three terms will carry you through most of the attachment literature you encounter in practice:
- Internal working models: Mental frameworks, built from early caregiving experiences, that shape how a person expects relationships to work. A child whose caregiver reliably responds to distress develops a model in which others can be trusted; one whose caregiver is inconsistent or absent builds a model built on uncertainty or self-reliance.
- Secure base behavior: A caregiver functions as a safe home base from which a child feels confident enough to explore the world, knowing they can return when frightened or overwhelmed.
- Proximity-seeking: The instinctive drive to move toward an attachment figure under stress. Understanding this drive helps social workers interpret behaviors that might otherwise look like defiance, clinginess, or withdrawal.
Why Social Workers Specifically Need This Framework
Attachment theory is not just background reading. It directly informs how social workers complete risk assessments, write case conceptualizations, design intervention plans, and provide expert testimony in child welfare court proceedings. When a worker can articulate why a child is showing particular behaviors in the context of attachment disruption, that reasoning carries clinical and legal weight.
How Attachment Theory Differs from Related Frameworks
Readers sometimes conflate attachment theory with object relations theory or social learning theory in social work. Object relations theory, rooted in psychoanalytic thought, also focuses on early relational experiences but centers on internalized representations of objects rather than observable proximity-seeking behaviors. Social work theories and practice models each offer a distinct lens; social learning theory explains behavior through reinforcement and modeling, without the biological and evolutionary scaffolding that Bowlby built into attachment theory. Placing these frameworks side by side helps social workers choose the right lens for each client situation rather than applying one theory to everything.
The Four Stages of Attachment Development
John Bowlby proposed that attachment does not appear fully formed at birth. Instead, it unfolds across four sequential stages, each building on the last. For social workers, these stages serve as a practical developmental map: knowing what to expect at a given age makes it easier to spot when something has gone wrong.
Stage 1: Pre-Attachment (Birth to 6 Weeks)
In the first weeks of life, infants respond to people in an undiscriminating way. They track faces, root toward caregivers, and use crying and grasping to signal need, but they do not yet prefer one person over another. Social workers assessing very young infants can observe whether caregivers respond consistently to these signals. An absence of caregiver responsiveness during this window is an early indicator of neglect risk.
Stage 2: Attachment in the Making (6 Weeks to 6-8 Months)
Infants begin to distinguish familiar caregivers from strangers, smiling more readily and settling more quickly in familiar arms. Eye contact becomes more sustained, and the infant starts to show anticipatory excitement when a known caregiver approaches. A child who has experienced frequent caregiver changes, such as multiple foster placements in rapid succession, may show flattened affect or indiscriminate friendliness rather than this emerging preference.
Stage 3: Clear-Cut Attachment (6-8 Months to 18-24 Months)
This is the stage most clinicians recognize as the heart of attachment formation. Three milestones are particularly useful for assessment:
- Separation protest: the child cries or protests when a primary caregiver leaves.
- Stranger anxiety: wariness or distress around unfamiliar adults, typically peaking around 8-10 months.
- Secure-base behavior: the child ventures away to explore but returns to the caregiver for reassurance.
Children who have spent extended time in institutional care or who have experienced chronic neglect often show delayed or absent stranger anxiety, which can be mistaken for easy temperament but warrants closer evaluation.
Stage 4: Formation of Reciprocal Relationships (18-24 Months Onward)
As language develops, children begin to understand that a caregiver's absence is temporary. They negotiate, make requests, and use words to influence a caregiver's behavior. Observable milestones include protest followed by comfort-seeking rather than inconsolable distress, and the ability to tolerate brief separations with a verbal explanation.
For child welfare social workers, this stage matters because disruptions, whether from institutionalization, abrupt placement changes, or parental incarceration, can delay the child's capacity to trust that relationships are reliable and manageable. These are normative stages under normative conditions. When conditions are far from normative, the stages can slow, stall, or take on distorted forms that require targeted intervention. Comparing these disruptions to how Erikson's psychosocial development theory maps trust and autonomy across early childhood can help practitioners build a fuller clinical picture rather than simply reassuring themselves that the child will catch up on their own.
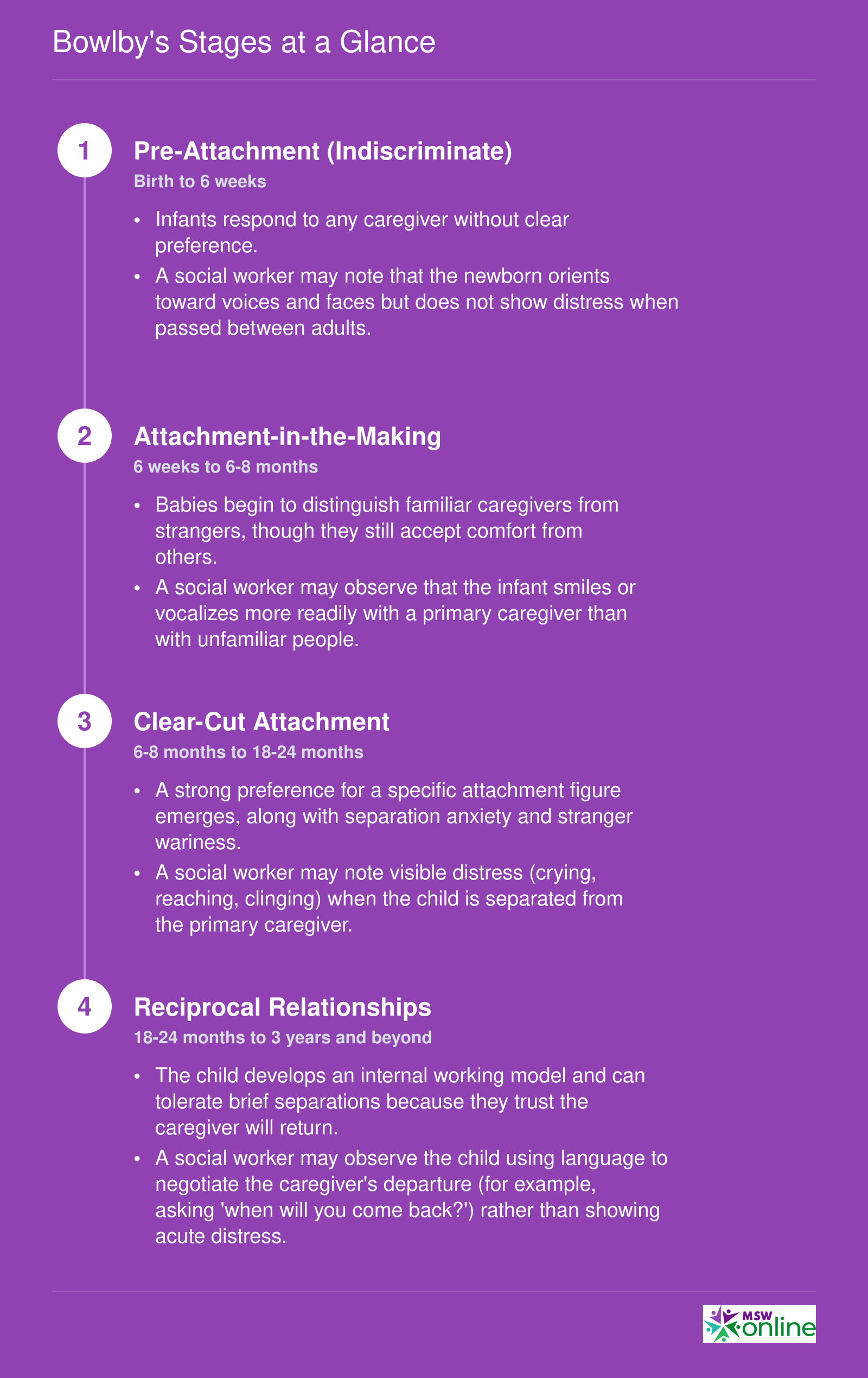
Bowlby's Stages at a Glance
John Bowlby described attachment as unfolding in a predictable sequence during the first few years of life. Each stage introduces new behaviors that signal how a child relates to caregivers. During assessment, social workers look for these observable markers to gauge a child's attachment development.
Attachment Styles: Secure, Insecure, and Disorganized
Since Mary Ainsworth's Strange Situation experiments in the 1970s, attachment classification has moved well beyond infancy research, becoming a core framework social workers use to understand adult behavior, relational patterns, and mental health risk across the lifespan. What began as a four-category model for toddlers now informs assessment and treatment planning in settings ranging from child welfare to substance-use recovery.
Secure Attachment
Approximately 51 to 62 percent of adults are classified as securely attached.1 In relationships, these individuals tend to be empathetic, comfortable with both intimacy and autonomy, and report high relationship satisfaction.2 From a clinical standpoint, secure attachment is associated with lower rates of depression, anxiety, and eating-disorder symptoms.3 In practice, social workers often treat secure attachment as a protective factor and a therapeutic goal: helping clients build the relational skills that mirror a secure base.
Anxious/Preoccupied Attachment
Roughly 11 to 20 percent of the population falls into the anxious or preoccupied category.1 Adults with this style frequently seek approval, experience chronic worry about abandonment, and may struggle to self-regulate in the face of perceived rejection.2 Research links anxious attachment to higher rates of social anxiety, insomnia, and depressive episodes.3 Social workers encounter this style often in crisis intervention and domestic-violence settings, where fear of abandonment can complicate safety planning.
Avoidant/Dismissive Attachment
Estimates place the avoidant or dismissive style at about 23 to 25 percent prevalence.1 These individuals emphasize self-reliance, downplay emotional needs, and report discomfort with closeness.2 While outwardly independent, they tend to score higher on measures of depression, anxiety, and loneliness.4 Social workers may notice avoidant patterns when clients resist engaging in services or minimize the severity of problems.
Disorganized/Fearful-Avoidant Attachment
The least common style, at roughly 5 percent of the population,1 disorganized attachment is also the most clinically significant. Adults in this category often have difficulty trusting others, display lower empathy, and behave unpredictably in relationships.2 This style carries the strongest associations with severe psychopathology, including increased risk for schizophrenia-spectrum presentations.3 In child welfare social work, disorganized attachment frequently surfaces in cases involving early trauma or caregiver abuse, making it a priority for assessment and intervention.
Understanding these four styles equips social workers to form more accurate case conceptualizations, select the right interventions, and anticipate the relational dynamics that will shape the therapeutic alliance. For broader context on how attachment fits within the wider body of social work theories and practice models, the theories hub offers a useful starting point.
Questions to Ask Yourself
Applying Attachment Theory Across Social Work Practice
Social workers apply attachment theory at every practice level, from one-on-one therapy to policy design. micro mezzo and macro social work each engage attachment frameworks differently: at the micro level, attachment shapes the therapeutic relationship itself; at mezzo, it guides family-level interventions and group services; at macro, it informs child welfare statutes and court protocols.
Micro Practice: The Therapeutic Alliance as Secure Base
Clinicians trained in attachment theory understand that the therapeutic relationship mirrors early caregiver bonds. A therapist becomes a temporary secure base from which a client explores painful memories, tests new relational patterns, and risks vulnerability. Research demonstrates that clients with insecure attachment styles, particularly avoidant and disorganized, face higher dropout rates in outpatient settings and report lower alliance quality in early sessions. Social workers address this by slowing rapport-building, naming ruptures explicitly, and maintaining consistent boundaries to establish predictability. The approach extends beyond child clients: adult-focused settings such as domestic violence services, substance use treatment, and geriatric social work increasingly adopt attachment lenses to understand clients' interpersonal patterns, emotional regulation deficits, and responses to loss in aging.
Mezzo Practice: Family and Group Interventions
Attachment theory shapes family-level work in multiple domains. Parent-child interaction therapy and similar dyadic models teach caregivers to recognize attachment cues, respond sensitively, and repair ruptures. In child welfare, kinship placement decisions weigh existing attachment bonds: a caseworker may prioritize a grandmother with whom a toddler has formed a secure attachment over a stranger foster home, even when logistical challenges exist. Group work for adoptive parents often centers attachment, normalizing the child's testing behaviors, teaching co-regulation strategies, and processing parental triggers when a child rejects comfort. These family interventions complement systems theory social work practice, which examines how the broader family system sustains or disrupts attachment security.
Macro Practice: Policy, Permanency, and Court Systems
Child welfare policy in the United States reflects attachment principles. The Adoption and Safe Families Act established permanency planning timelines, typically twelve months, because prolonged placement instability disrupts attachment formation. Placement stability mandates and sibling co-placement requirements aim to preserve existing bonds. Social workers testifying in dependency court cite attachment assessments to support reunification or termination recommendations, arguing that a child's secure attachment to a foster parent may outweigh biological ties when reunification efforts have failed.
Case Vignette: Disorganized Attachment in Foster Care
A social worker assesses Maya, a three-year-old in her fourth placement within eighteen months. During visits, Maya approaches her foster mother, then freezes mid-step, backing away while maintaining eye contact. She does not seek comfort after a minor fall. The worker recognizes disorganized attachment, a pattern often linked to maltreatment. Assessment using the Strange Situation classification confirms the pattern. Case conceptualization centers on placement stability and trauma-informed caregiving. The intervention recommendation: maintain the current foster placement, enroll the dyad in attachment-focused therapy, and delay another move to allow secure-base development.
Expanding Applications Beyond Child Welfare
Attachment theory now informs practice with adults across settings. Domestic violence advocates explore how insecure attachment predicts relationship violence and help-seeking patterns. Substance use counselors address how avoidant attachment correlates with emotional numbing through substances. Geriatric social workers apply attachment frameworks to understand grief, isolation, and resistance to care transitions in older adults, recognizing that nursing home placement can trigger attachment distress similar to childhood separation.
Related Articles
Assessment Tools Social Workers Use to Evaluate Attachment
Inter-rater reliability coefficients of .70 or higher are the baseline threshold for every major attachment assessment instrument in clinical use, yet each tool differs significantly in its target population, training requirements, and what it actually captures.1 Social workers selecting an assessment must match the tool to the client, the practice setting, and their own credentialing.
Strange Situation Procedure (SSP)
Developed by Mary Ainsworth, the SSP is the foundational laboratory measure of infant attachment. It classifies infants aged 12 to 20 months into secure, avoidant, resistant, or disorganized categories based on observed reunion behavior with a caregiver after brief separations.1 Inter-rater kappa values reach .80 or above for three- and four-way classifications, and decades of research have produced extensive validity evidence. The SSP requires a controlled lab environment, making it most common in university-affiliated research clinics rather than field-based child welfare work. Administration requires a graduate degree (an MSW qualifies) plus completion of a recognized SSP coding course and demonstrated inter-rater reliability.
Adult Attachment Interview (AAI)
The AAI is a semi-structured interview for adults that evaluates state of mind regarding early attachment experiences, scoring for coherence, idealization, and related dimensions.1 Inter-rater kappa ranges from .70 to .90 for the four-way classification system, with strong construct and predictive validity. Clinical social workers in mental health, forensic, and family reunification settings use the AAI to inform treatment planning. Administering and coding the AAI requires a graduate degree (MSW, PhD, or equivalent) plus official AAI coding training and reliability certification.
CARE-Index
Designed for infants from birth through 15 months, the CARE-Index assesses the caregiver-infant dyad rather than the child alone. It measures caregiver sensitivity, control, and unresponsiveness alongside infant cooperation, compulsive behavior, difficult behavior, and passivity.1 Inter-rater intraclass correlation coefficients fall between .70 and .85 on key scales, and the tool has demonstrated concurrent and predictive validity. It is well suited for early intervention programs, home visiting services, and child protective services. Professionals need a qualifying degree such as an MSW plus formal CARE-Index training and reliability testing.
Attachment Q-Sort (AQS)
The AQS provides a continuous security score for children aged 12 to 48 months, making it useful when a categorical label is less informative than a dimensional measure. Trained observers sort 90 behavioral descriptors after watching the child in a naturalistic setting, typically the home.1 Inter-rater correlations for security scores are .70 or higher, and the AQS shows moderate concurrent validity with the SSP (correlations in the .30 to .40 range). Social workers conducting in-home assessments or family preservation evaluations find the AQS practical because it does not require a laboratory. Master's-level training in child development and specific AQS reliability training are prerequisites.
Marschak Interaction Method (MIM)
The MIM is a structured observation tool for parent-child dyads across a wide age range. It evaluates interactive behaviors along four dimensions: attachment, engagement, challenge, and nurturing.1 Inter-rater intraclass correlation coefficients reach .70 or above for global dimensions, though the overall psychometric evidence base remains more limited than that of the SSP or AAI. The MIM is most commonly used within Theraplay-informed practice settings, including outpatient family therapy and therapeutic foster care programs. Clinicians must hold a master's-level mental health degree and complete Theraplay Level 1 certification along with dedicated MIM training.
Choosing the Right Tool
When selecting an attachment assessment, consider three factors:
- Client age: The SSP and CARE-Index serve infants; the AQS extends into toddlerhood; the MIM spans childhood; the AAI targets adults.
- Setting constraints: Laboratory-based tools like the SSP are impractical in most field settings, whereas the AQS and MIM work well in homes and community agencies.
- Credential requirements: Every tool demands specialized training beyond a graduate degree, so agencies should budget for staff certification and ongoing reliability checks.
Social workers preparing for the ASWB exam prep should be familiar with these instruments by name and purpose, even if day-to-day practice involves only one or two of them.
Evidence-Based Attachment Interventions: A Comparison
Choosing the right attachment intervention requires more than familiarity with a model. Social workers must weigh the client's age, the nature of the attachment disruption, the practice setting, and what training they have completed or can realistically access. The five interventions below represent the strongest options in current practice, though their evidence bases vary considerably. Selecting a well-supported intervention for your specific population is always preferable to defaulting to a familiar one that may not fit the clinical picture.
Attachment and Biobehavioral Catch-up (ABC)
ABC is the most rigorously studied intervention in this group. Designed for infants and toddlers under three years old who have experienced maltreatment, neglect, or placement in foster care, it uses a structured ten-session home-visiting format in which a trained coach works directly with the caregiver. Multiple randomized controlled trials have demonstrated its effectiveness in reducing disorganized attachment behaviors, improving cortisol regulation, and increasing caregiver sensitivity.1 For social workers in child welfare, foster care, or early intervention settings, ABC should be a first-line consideration when working with high-risk infants and toddlers.
Video Interaction Guidance (VIG)
VIG uses short clips of video recorded during parent-child interaction as the basis for guided reflection with the caregiver. The practitioner reviews the footage with the parent, drawing attention to moments of successful attunement. Like ABC, it targets infants and toddlers in at-risk or community samples, and it carries strong RCT support.1 VIG fits naturally into community health, home visiting, and early childhood programs where capturing brief video interactions is feasible.
Circle of Security
Circle of Security is delivered in a group format, most often with foster caregivers or parents of infants and preschoolers. It teaches caregivers to read children's attachment cues and to serve as a reliable secure base. The evidence base is moderate, with studies showing improvements in caregiver sensitivity and reductions in insecure attachment classifications.2 Its group structure makes it cost-effective for early childhood centers and foster carer support programs.
Dyadic Developmental Psychotherapy (DDP) and Theraplay
Both DDP and Theraplay serve older children and have more limited research support compared to the interventions above. DDP is designed for school-age children with complex trauma and adoption or foster care histories, and it is delivered in clinical settings by specially trained therapists. Reviews of DDP published in peer-reviewed psychological journals note promising clinical outcomes but call for more rigorous trial designs before strong efficacy claims can be made.3
Theraplay uses structured play activities to build attunement, self-esteem, and regulation between child and caregiver, and is suited for preschool and early school-age children with social or attachment difficulties in clinical or special needs settings.4 Like DDP, it currently rests on a limited evidence base, though clinical experience and theoretical coherence support its continued use where better-evidenced options are unavailable or impractical. Understanding how these interventions align with broader social work practice models can help practitioners frame their selection within a coherent theoretical rationale.
Choosing Among the Options
As a practical guide:
- ABC: Best for infants and toddlers in child welfare or foster care; requires certified coach training.
- VIG: Best for at-risk infants and toddlers in community or home-visiting contexts; requires practitioner training in the VIG model.
- Circle of Security: Best for foster carer groups and early childhood settings; group-based and more accessible for agencies without specialist training budgets.
- DDP: Best for school-age children with complex trauma and foster or adoptive placement histories; requires specialized clinical training.
- Theraplay: Best for preschool and early school-age children with regulation or relational difficulties in clinical or special needs contexts; requires Theraplay Institute training.
When in doubt, match intervention to evidence strength first, then to your setting and training capacity.
Use attachment assessment to inform clinical thinking, not to dictate it. A disorganized classification is a signal that warrants deeper exploration, not a fixed diagnostic label. Always interpret findings within the child's full developmental history, family system, and cultural context, and pair observations with collateral information before shaping any intervention plan.
Strengths, Criticisms, and Cultural Considerations
Attachment theory remains one of the most empirically supported frameworks in developmental psychology, yet the field continues to debate its boundaries, measurement tools, and cultural reach.
What the Theory Gets Right
Attachment theory's greatest strengths are its empirical foundation and its practical utility. Bowlby grounded his ideas in observable behavior and biology, and Ainsworth followed with structured research methods that made attachment patterns measurable. Decades of longitudinal studies have linked early attachment quality to outcomes in mental health, relationships, and social functioning, giving social workers a research-backed rationale for early intervention. The theory also translates well across practice settings, from child welfare assessments to trauma-informed therapy to community-based parenting programs.
Another strength is explanatory depth. Attachment theory can account for why adults who experienced childhood neglect may struggle to trust helping relationships, which has direct implications for how social workers build rapport and pace their work with clients.
Criticisms Worth Knowing
No theory is without limits, and attachment theory has attracted serious critique on several fronts.
- Cultural universality: Ainsworth's original work was conducted in Western, primarily middle-class samples. Cross-cultural research, including large-scale meta-analyses by scholars such as van IJzendoorn and colleagues, has found that secure attachment appears across cultures as the most common pattern, but the distribution of insecure styles varies in ways that reflect cultural norms around caregiving and independence. A behavior classified as avoidant in one cultural context may simply reflect a different but adaptive caregiving tradition.
- Maternal focus: Early formulations placed heavy emphasis on the mother as the primary attachment figure, undervaluing fathers, extended family, and community caregiving structures common in many non-Western societies.
- Category rigidity: Critics argue that Ainsworth's four-category classification system may oversimplify a spectrum of attachment behavior. Patricia Crittenden's Dynamic-Maturational Model offers an alternative framework that emphasizes how attachment strategies evolve across the lifespan in response to ongoing experience, rather than remaining relatively stable after early childhood. The DMM has attracted both scholarly interest and debate, with ongoing discussion about how it compares to the standard model in clinical and child welfare contexts.
Implications for Social Work Practice
For practitioners, these criticisms are not reasons to abandon the theory but reasons to apply it carefully. Assessing attachment should always include attention to a family's cultural background, caregiving structure, and community context. Social workers who treat attachment classifications as fixed diagnoses rather than working hypotheses risk misreading adaptive coping strategies as pathology. Awareness of cultural considerations in Erikson's theory offers a useful parallel: just as developmental stage frameworks require cultural humility, so too does attachment assessment. Professional bodies such as NASW encourage ongoing education in culturally responsive practice, and continuing education modules comparing attachment models are widely available through academic and professional association channels.
Used with appropriate humility, attachment theory is a powerful lens. Used without it, the same theory can pathologize difference.
Cross-cultural research reveals that secure attachment is far from universal. A large-scale meta-analysis found that only 52% of children worldwide display secure attachment patterns, with rates varying significantly across cultures. This challenges early assumptions that attachment theory operates identically in all societies and underscores the importance of cultural context in assessment and intervention.
Attachment Theory and the ASWB Licensing Exam
Studying independently with scattered internet resources versus preparing with official materials from the licensing body: this choice can make or break your ASWB exam performance. Social work candidates often piece together study notes from forums or outdated prep books, but the most reliable path to understanding what the exam covers, including how attachment theory shows up, is to go straight to the source.
Finding Reliable Information About the ASWB Exam
The Association of Social Work Boards (ASWB) publishes detailed test content outlines for each exam level: Bachelors, Masters, and Clinical. These outlines are publicly available on the ASWB website and serve as the definitive blueprint for what may appear on your exam. Within them, you will find broad domains like Human Development, Diversity, and Behavior in the Environment, areas where attachment theory naturally fits. Rather than memorizing isolated facts, candidates should understand how attachment concepts relate to developmental milestones, family systems, and client relationships.
To stay current, always check the ASWB website for the latest content outlines, as they undergo periodic updates. Professional social work associations, such as the National Association of Social Workers (NASW), also offer guidance on exam preparation and may highlight key theoretical frameworks. While test-prep companies can provide structure, verify any third-party material against the official outlines to avoid studying outdated or inaccurate content.
Where to Locate Official Content Outlines
- Visit the ASWB website (aswb.org) and navigate to the "Exam Candidates" section.
- Download the candidate handbook for your specific exam level. The handbook includes the content outline, sample questions, and test-taking policies.
- Use the outline as a checklist during your review: each knowledge, skill, and ability statement signals a topic you may encounter.
Many accredited social work programs also embed ASWB test preparation into their curriculum. Reach out to your program's field education office or academic advisor, as they can often point you to school-specific resources or study groups. If you are an online student, your institution's student portal or library may have curated exam prep modules.
How Attachment Theory Typically Appears on the Exam
While the ASWB does not disclose the exact number of questions on any one theory, attachment theory commonly appears within questions about child and adolescent development, caregiver-child interactions, and relationship-based practice. You might be asked to identify attachment styles based on a case vignette, recommend interventions informed by attachment principles, or recognize indicators of disrupted attachment in a family assessment.
Because exam questions often present real-world scenarios, a conceptual grasp of Bowlby's and Ainsworth's work is more valuable than rote memorization. Expect to apply attachment theory to differentiate between secure, insecure, and disorganized patterns, and to understand how these patterns influence client functioning across the lifespan.
Study Strategies for Theory-Based Exam Content
- Start by reviewing official outlines to see which developmental and behavioral theories are listed. Even if attachment theory is not named explicitly, it falls under broader headings like "Theories of Human Development" or "Theories of Attachment and Bonding."
- Use reputable textbooks and peer-reviewed articles recommended by your social work faculty. Government sources like the Child Welfare Information Gateway (childwelfare.gov) provide free, evidence-based resources on attachment that align with exam expectations.
- Practice with sample questions that require you to analyze a brief client scenario and choose the most appropriate theory-based response. This mirrors the application-heavy format of the ASWB exam.
- Form or join a study group where you can discuss how attachment theory intersects with other frameworks, because the exam often tests integrated knowledge.
If your studies include ASWB Masters exam content, reviewing how human development theories are categorized within the LMSW content outline is a practical starting point. Understanding where attachment theory sits alongside frameworks such as Erikson's stages of psychosocial development helps you build the kind of integrated theoretical knowledge the exam rewards. Finally, before you sit for the exam, double-check the ASWB site one last time to ensure your study materials still match the current structure. By anchoring your preparation in official sources, you move beyond guesswork and build a strategic, high-confidence approach to the test.
Frequently Asked Questions About Attachment Theory in Social Work
Below are answers to common questions about attachment theory and its role in social work education, practice, and licensure. These responses offer concise starting points; each topic is explored in greater depth in the sections above.
Explore More
- Ecological Systems Theory in Social Work
- Erikson's Psychosocial Development Theory in Social Work
- Psychodynamic Theory in Social Work
- Rational Choice Theory in Social Work
- Social Exchange Theory in Social Work
- Social Learning Theory in Social Work
- Strengths-Based Perspective in Social Work
- Systems Theory in Social Work