Points of interest…
- Dennis Saleebey codified six core principles at the University of Kansas in the early 1990s that still anchor strengths-based practice today.
- A 2023 meta-analysis found a small but consistent effect size of 0.17 for strengths-based psychotherapies across multiple studies.
- The ASWB licensing exam tests the strengths perspective across several content areas, making it essential study material for MSW candidates.
- Critics caution that overemphasizing strengths can minimize real risks, so practitioners should integrate the model with complementary frameworks.
Dennis Saleebey's landmark text "The Strengths Perspective in Social Work Practice" has gone through six editions since its 1992 debut, a publishing arc that reflects how thoroughly this orientation has reshaped mainstream practice.
The strengths-based perspective is a practice orientation that centers client capabilities, resilience, and existing resources rather than cataloging deficits or pathology. Where the traditional deficit model asks what is broken and who is to blame, the strengths perspective asks what clients already know, what they have survived, and what they want to build. That contrast is not merely philosophical. It changes assessment language, interview technique, goal-setting, and the power dynamic between practitioner and client.
In 2026, ASWB content outlines, MSW accreditation standards, and agency practice models increasingly treat strengths-based orientation as a baseline competency rather than an elective philosophy. Social workers who cannot articulate both its principles and its limitations are at a real disadvantage in licensing exams, job interviews, and clinical supervision. This guide covers the perspective's origins, social work practice models it intersects with, its application across all levels of practice, and its place on the ASWB licensing exam.
Origins and Key Theorists: From the University of Kansas to Mainstream Practice
The strengths-based perspective did not emerge from a single eureka moment. It developed gradually through the work of social work educators and practitioners who grew frustrated with a field that had become increasingly focused on diagnosing problems rather than building on what people already had going for them.
Dennis Saleebey and the Kansas Foundation
The most recognized architect of the strengths perspective is Dennis Saleebey, a professor at the University of Kansas School of Social Welfare. His 1992 edited volume, "The Strengths Perspective in Social Work Practice," gave the framework its first formal, book-length articulation. Saleebey argued that social work had drifted too far toward pathology, cataloguing what was wrong with clients rather than what was possible for them. His framework offered six organizing principles that repositioned clients as capable individuals with inherent resources, rather than passive recipients of professional fixes. The University of Kansas became the intellectual home base for this rethinking, with Saleebey and his colleagues continuing to refine the approach through subsequent editions of that foundational text.
Charles Rapp and Strengths-Based Case Management
Running parallel to Saleebey's theoretical work was the applied research of Charles Rapp, also at the University of Kansas. Rapp developed a strengths-based model of case management specifically for people living with severe mental illness. Rather than organizing services around symptom management and deficits, Rapp's model asked what goals the client valued and what community resources could be mobilized in support of those goals. His research showed measurable improvements in housing stability, employment, and quality of life, giving the perspective an early empirical foothold at a time when it might otherwise have been dismissed as idealism.
A Reaction to Deficit Dominance
To understand why this framework resonated, you have to appreciate the climate it pushed back against. The 1980s and early 1990s saw the Diagnostic and Statistical Manual expand dramatically in scope, and managed care pressures pushed practitioners toward rapid assessment and label-first thinking. The broader positive psychology movement, emerging through researchers like Martin Seligman, reinforced the idea that human flourishing deserved as much scientific attention as dysfunction. The strengths perspective sat at the intersection of these currents, offering social work a language and a set of practice principles that fit the profession's core values far better than the medical model did. It is worth noting how differently this orientation reads when placed alongside social work theories and practice models more rooted in pathology or behavioral deficits.
From Kansas to National Policy
What began as a regional academic initiative eventually found its way into NASW practice standards and CSWE accreditation requirements. Today, accredited MSW programs across the country are expected to teach students how to identify and mobilize client strengths. The perspective is no longer a fringe alternative to mainstream practice; it is mainstream practice, embedded in syllabi, licensing exam content, and agency training programs nationwide.
The Six Core Principles of the Strengths Perspective
What are the six principles of the strengths perspective? Dennis Saleebey, the scholar most closely associated with codifying the strengths-based perspective in social work, identified six foundational principles that distinguish this approach from traditional deficit-focused models. While some authors condense these into four or five broader themes, Saleebey's six-principle framework remains the canonical formulation taught in most MSW programs and tested on the ASWB licensing exam. Each principle reshapes how practitioners view clients, build relationships, and intervene at every level of practice.
1. Every Individual, Group, Family, and Community Has Strengths
The first principle asserts that all human systems possess inherent capacities, talents, and resources, no matter how dire their circumstances appear. Practitioners are trained to look beyond presenting problems and actively identify what clients do well, what they care about, and what has worked in the past. For example, a social worker meeting a family experiencing homelessness might discover that the parents have successfully kept their children enrolled in school, maintained a daily routine, and cultivated a network of supportive friends at a local shelter. These existing strengths become the foundation for housing-stability interventions rather than starting from a list of deficits.
2. Trauma and Adversity Can Also Be Sources of Challenge and Opportunity
Saleebey's second principle acknowledges that while hardship is painful, it can also catalyze resilience, insight, and growth. This does not minimize suffering or suggest that trauma is beneficial; rather, it recognizes that people often develop profound coping skills, empathy, and wisdom through surviving difficult experiences. A clinical social worker supporting a survivor of intimate-partner violence might explore how the client's journey through the legal system or shelter system has revealed courage, problem-solving ability, or a renewed commitment to safety and autonomy. These insights inform trauma-informed care that honors both the wound and the wisdom.
3. Assume You Do Not Know the Upper Limits of a Client's Capacity to Grow
The third principle guards against professional hubris and diagnostic pessimism. Practitioners are urged never to foreclose on a client's potential based on labels, history, or external judgments. A school social worker, for instance, might work with a student labeled as having a severe learning disability and behavioral issues. Rather than setting low expectations, the social worker collaborates with teachers and family to identify the student's unique interests (perhaps art or mechanics), creates individualized supports, and remains open to outcomes that exceed initial projections. This principle underpins person-centered planning and recovery-oriented mental health practice.
4. Practitioners Best Serve Clients by Collaborating With Them
The fourth principle repositions the social worker as a partner rather than an expert who diagnoses and prescribes. Clients are regarded as the experts on their own lives, and meaningful change emerges from genuine collaboration and shared decision-making. In a community mental health setting, a social worker might co-create a wellness recovery action plan with a client living with schizophrenia, asking the client to identify personal warning signs, preferred coping strategies, and trusted supporters. This collaborative stance respects autonomy, builds engagement, and leads to more sustainable outcomes.
5. Every Environment Is Full of Resources
Saleebey's fifth principle shifts attention from what is missing in a client's environment to what is already present but underutilized. Communities, no matter how under-resourced, contain informal networks, cultural practices, faith communities, parks, libraries, neighbors, and voluntary organizations. A hospital social worker arranging discharge for an elderly patient might map out the patient's neighborhood and discover a nearby senior center, a volunteer transportation service, and a retired nurse who lives two doors down and is willing to check in daily. Recognizing environmental assets enables more creative, less costly, and more community-embedded interventions. This environmental lens closely parallels concepts found in ecological systems theory in social work, which also encourages practitioners to assess the full range of systems surrounding a client.
6. Caring, Caretaking, and Context Matter
The sixth principle emphasizes that relationships, culture, and social context profoundly shape well-being and that effective practice must attend to these dimensions. Social workers are called to create warm, respectful, and hopeful therapeutic alliances and to understand clients within their full ecological and cultural contexts. A child welfare worker, for example, might learn that a grandmother caring for her grandchildren draws strength from her role as family matriarch and from rituals rooted in her Indigenous heritage. By honoring those relational and cultural contexts rather than pathologizing non-nuclear family structures, the social worker supports the family's stability and identity.
Variations in the Literature
While Saleebey's six-principle framework is most widely cited, readers should be aware that some texts consolidate these into fewer principles or emphasize different aspects. Rapp and Goscha, for instance, highlight four principles in their strengths model of case management, and other authors foreground resilience or empowerment as overarching themes. These variations reflect evolving scholarship rather than contradictions, and all share the core commitment to recognizing and mobilizing client capacities. For exam preparation and coursework, familiarity with Saleebey's canonical six remains essential.
Strengths Vs. Deficit Model: A Side-By-Side Comparison
Social workers often face a fundamental choice: approach clients by cataloging their problems and gaps, or by identifying their capacities and resources. This decision shapes not only the therapeutic relationship but also measurable outcomes in motivation, competence, and long-term change. The strengths-based perspective and the deficit (or medical) model represent two distinct philosophies, each with its own guiding questions, assumptions, and implications for practice.
Core Differences in Focus and Framing
The strengths-based perspective asks, "What is present that we can build upon?" and directs attention to existing strengths, assets, and capacities.1 The deficit model, rooted in medical and diagnostic traditions, asks, "What is missing that we must go find?" and centers on weaknesses, problems, lacks, and deficits.2 These divergent starting points shape every subsequent interaction, from assessment to goal-setting to discharge planning.
Performance and Competence Outcomes
Research comparing the two approaches reveals consistent patterns. In workplace settings, strengths-based interventions show positive correlations with both self-rated and manager-rated job performance, whereas deficit correction strategies show no significant relation to either measure.3 In educational and training contexts, students exposed to strength-based feedback report higher perceived competence, higher intrinsic motivation, and higher effort intentions than peers receiving deficit-focused feedback.4 These differences are not marginal; they reflect fundamentally different paths to engagement and efficacy.
Equity, Empowerment, and Community Practice
The models carry distinct equity implications. Strengths-based practice treats diversity as an asset, recognizing cultural resources, community networks, and resilience forged through adversity.5 The deficit model, by contrast, can reinforce bias toward marginalized groups by framing difference as deviation or lack.5 At the community level, strengths-based approaches are associated with empowerment and sustainable change, while deficit-focused interventions risk burnout, dependency, and downward spirals.1 Psychologically, individuals engaged through a strengths lens report hope, growth, resilience, and agency; those subjected to persistent deficit framing may experience helplessness and low expectations.6
Selecting the Right Lens
No single model suits every situation. Crisis intervention and acute symptom management may require deficit-focused diagnostic precision, while longer-term rehabilitation, community organizing, and educational settings benefit from strengths-based engagement. The most effective practitioners learn to toggle between lenses, using deficit assessments to identify urgent needs and strengths assessments to chart pathways forward. Across social work theories and practice models, this interplay between problem-focused and asset-focused frameworks is a recurring theme. Understanding these contrasts prepares social workers to choose tools intentionally, grounded in evidence and aligned with the values of self-determination and social justice.
Questions to Ask Yourself
How the Strengths-Based Perspective Is Applied: Micro, Mezzo, and Macro Practice
Deficit-focused practice asks "what is wrong and how do we fix it?" Strengths-based practice asks "what is working, what does the client want, and what resources can we mobilize to get there?" That single reframing changes how social workers operate at every level of intervention. To apply a strengths-based approach, you systematically identify capacities, collaborate on client-defined goals, document progress in strengths language, and connect individuals or communities to existing assets rather than only to remedial services. The shape of that work shifts as you move across the social work theories micro mezzo macro levels of practice.
Micro Practice: A Case Vignette
Consider Maria, a 29-year-old single mother of two recently housed after eight months in a shelter. A deficit-oriented intake would catalog her unemployment, eviction history, and untreated anxiety. A strengths-based intake covers those concerns but goes further. The social worker asks Maria what kept her and her children safe during the shelter stay, what skills she used to navigate the housing waitlist, and what she wants the next twelve months to look like.
Maria identifies persistence, a tight relationship with her sister, two years of medical billing experience, and a goal of returning to community college. The practitioner co-writes goals using Maria's language: "reconnect with my billing certification program by September" rather than "address vocational deficit." Progress notes record observable strengths in action: "client independently scheduled three appointments and arranged childcare with her sister." Referrals flow toward asset-building resources (a workforce program, a parenting group she chose) rather than only crisis services.
Mezzo Practice: Groups and Organizations
At the group and organizational level, the strengths perspective shapes how programs are designed and facilitated. A support group for veterans, for example, might open each session by inviting members to name a coping skill they used that week. The facilitator builds peer mentorship into the structure, treating long-time members as experts rather than patients. Organizationally, agencies can audit their intake forms, supervision practices, and outcome measures to ensure they capture client capacities, not just risk factors.
Macro Practice: Community and Policy
Most discussions of the strengths perspective stop at the individual, but its macro applications are substantial. Asset-Based Community Development (ABCD), developed by Kretzmann and McKnight, treats neighborhoods as inventories of skills, associations, institutions, and physical assets rather than as bundles of needs. This approach complements systems theory in social work, which similarly emphasizes the interconnected resources and relationships surrounding a client.
Practical macro applications include:
- Community asset mapping: Engaging residents to document local skills, businesses, faith communities, and informal networks that can anchor new initiatives.
- Policy advocacy grounded in community voice: Centering testimony from directly affected residents when advocating for housing, immigration, or criminal justice reform.
- Participatory budgeting and coalition building: Structuring decisions so community members co-design solutions rather than receive them.
Applied consistently across all three levels, the strengths perspective becomes less a technique and more a stance the social worker brings to every encounter.
Related Articles
Strengths-Based Assessment Tools and Techniques
What assessment tools are used in strengths-based social work? Practitioners have several validated instruments to choose from, and selecting the right one depends on the client population, practice setting, and purpose of the assessment.
Validated Instruments at a Glance
The table below summarizes tools with published psychometric support that align with strengths-based values.
| Instrument | Author(s) / Era | Target Population | Practice Context |
|---|---|---|---|
| Child and Adolescent Needs and Strengths (CANS) | John S. Lyons and colleagues, late 1990s | Children and youth ages 6-20 | Behavioral health, child welfare, juvenile justice |
| Behavioral and Emotional Rating Scale (BERS-2) | Epstein, 2004 | Children and youth | School-based and mental health settings |
| VIA Character Strengths Survey | Peterson and Seligman, 2004 | Adults and adolescents | Counseling, coaching, community practice |
| Strengths Assessment Worksheet | Rapp and Goscha, 2006 | Adults with serious mental illness | Case management, psychiatric rehabilitation |
| Solution-Focused Goal Attainment Scale | Multiple adaptations | Adults and families | Brief therapy, community mental health |
The CANS is one of the most rigorously studied options in this group.1 Interrater reliability coefficients range from 0.78 using vignettes to 0.84 with case records, and reach 0.90 or above when trained raters work with live cases.2 Total scores have demonstrated the ability to distinguish appropriate levels of care, and scores predict service utilization and costs over time.2 Practitioners are required to complete initial training and annual recertification to maintain scoring accuracy.3 One caution: a recent psychometric review found inconsistent internal consistency and factor loadings across subdomains,4 so the CANS is best interpreted at the domain level rather than as a single composite score.
Saleebey's Five Question Types for Strengths-Based Interviewing
Beyond formal instruments, Dennis Saleebey outlined five categories of interview questions that guide practitioners toward identifying strengths rather than cataloguing deficits. These question types connect naturally to psychodynamic assessment in social work, which also relies on open-ended inquiry, though the two frameworks differ sharply in what they are trying to surface.
- Survival questions: These invite clients to reflect on how they have coped. Example: "You have been dealing with housing instability for over a year. What has kept you going?"
- Support questions: These surface natural helpers and community resources. Example: "Who in your life has shown up for you during hard times, even in small ways?"
- Exception questions: These look for periods when the problem was less severe. Example: "Can you think of a time recently when things felt a little more manageable? What was different?"
- Possibility questions: These orient clients toward future aspirations. Example: "If things were going the way you hoped, what would your life look like six months from now?"
- Esteem questions: These affirm capacity and invite pride. Example: "What is something you have done in the past few months that you feel good about, even if it seems small?"
Using these question types consistently shifts the tone of an intake or ongoing session and often surfaces information that a deficit-focused interview would miss entirely.
Documenting Strengths in Case Notes and Treatment Plans
Recording strengths is not simply a clinical courtesy. Many state licensing boards and accreditation bodies now expect strengths to appear alongside diagnostic information in formal documentation. In practice, this means a treatment plan should include a dedicated strengths section that lists specific client capacities, supports, and past successes, not just a diagnosis and a list of presenting problems.
In case notes, practitioners can apply a modified SOAP or DAP format by adding a brief strengths observation to each entry. For example, after documenting a client's continued struggle with medication adherence, a practitioner might note that the client independently identified two personal motivators for staying on a regimen and arrived on time for three consecutive appointments. These observations create a longitudinal record of capacity that informs both clinical decision-making and advocacy conversations with insurance reviewers or courts.
Did you know a 2023 meta-analysis of strength-based psychotherapies found an overall effect size of 0.17? While small, this indicates consistent, measurable client improvements across studies, suggesting that systematically building on a person's assets can quietly shift mental health outcomes in the right direction.
What the Evidence Says: Empirical Outcomes of Strengths-Based Practice
Social work's embrace of strengths-based practice has outpaced the research base needed to validate it, creating a gap that researchers are working to close with varying degrees of success. While the conceptual appeal is broad, empirical evidence remains concentrated in a few practice areas, primarily mental health, with substantial gaps in child welfare, aging services, and community organizing.
Strongest Evidence: Mental Health and Psychotherapy
A 2023 systematic review and meta-analysis by Fluckiger and colleagues examined strengths-based psychotherapies across nine randomized trials (57 effect sizes).1 Compared to active control conditions, strengths-based interventions demonstrated a small but statistically significant effect (Hedges' g = 0.166, 95% CI 0.027-0.305).1 This pooled finding suggests that when clients receive psychotherapy explicitly framed around identifying and mobilizing personal strengths, they experience modestly better outcomes than those in comparison treatments. The magnitude is clinically meaningful in aggregate, though smaller than effect sizes reported for well-established cognitive or behavioral therapies.
Emerging Evidence in Workplace and Organizational Settings
Strengths-based interventions have migrated beyond clinical social work into organizational psychology, where the evidence base is also developing. A 2022 meta-analysis by Gander and colleagues focused on character strengths interventions in workplace settings, finding a small to moderate effect on work engagement (Cohen's d = 0.27, 95% CI 0.05-0.49) across six effect sizes and 452 participants.2 A 2018 pre-registered meta-analysis by van Woerkom and colleagues similarly concluded that strengths-use interventions in organizations yield small to moderate effects.3 While these studies do not involve social work practitioners directly, they inform strengths-based practice in employee assistance programs, workplace wellness, and vocational rehabilitation.
The Evidence Gap in Core Social Work Domains
Outside of mental health, the empirical base thins considerably. A 2023 National Institute for Health Research review of strengths-based models in social work research and practice rated the overall evidence quality as insufficient.4 The review identified a scarcity of randomized controlled trials, reliance on quasi-experimental designs, and inconsistent outcome measurement. Research in child welfare, substance use treatment, and gerontological social work remains largely observational or anecdotal, with few comparison-group studies and limited follow-up periods. A 2023 consensus study published in a SAGE journal sought to standardize outcome measures for evaluating strengths-based approaches, signaling both the potential for future rigorous trials and the current lack of uniformity in how success is defined.5
Study Design Limitations
Most published studies are non-randomized, often comparing programs before and after implementation of strengths-based principles or comparing clients who opt into strengths-oriented services against those who do not. These designs cannot rule out selection bias or confounding. When randomized trials do exist, they frequently compare strengths-based interventions to waitlist controls rather than active alternative treatments, inflating apparent effect sizes. The field needs more head-to-head trials, longer follow-up windows, and replication across diverse populations and service settings to establish strengths-based practice as an evidence-based intervention in the full range of social work contexts.
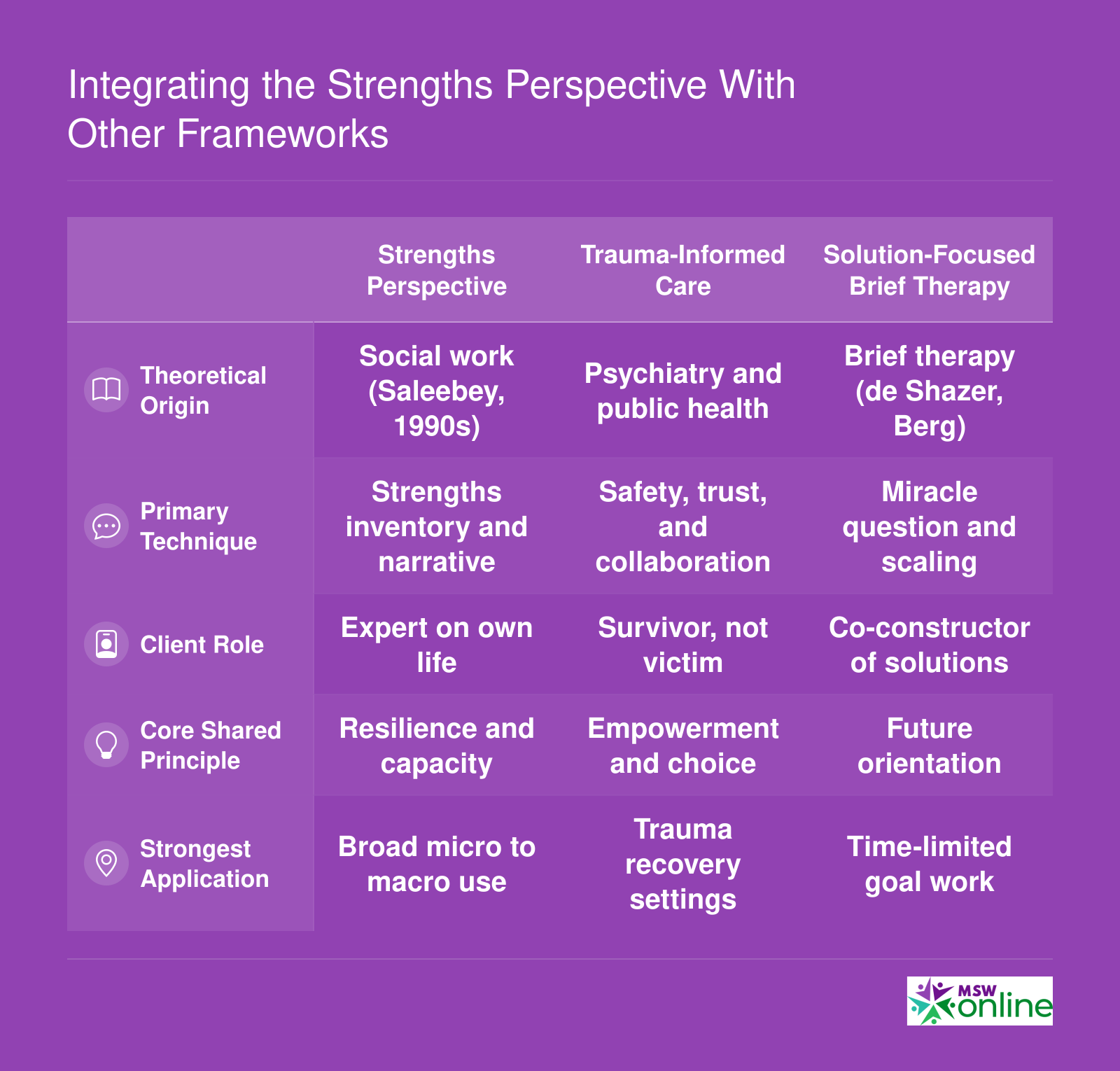
Integrating the Strengths Perspective With Other Frameworks
Practitioners rarely use the strengths perspective in isolation. Trauma-informed care, solution-focused brief therapy, and motivational interviewing each share philosophical DNA with the strengths-based approach, yet they differ in origin, technique, and optimal setting. A clinician conducting a strengths-based assessment, for example, might draw on motivational interviewing's open-ended questioning style to surface a client's internal resources, or layer trauma-informed principles to ensure the conversation does not inadvertently re-traumatize. In mental health settings, the recovery model aligns closely with the strengths perspective by centering hope, self-determination, and the belief that people can build meaningful lives beyond a diagnosis. Understanding where these frameworks overlap and diverge helps practitioners combine them intentionally rather than haphazardly.
Cultural Competence, Anti-Oppressive Practice, and the Strengths Perspective
The strengths perspective aligns naturally with culturally responsive social work because it begins with the client's own definition of strength. Rather than measuring someone against a dominant-culture template of wellness or success, the framework asks practitioners to follow the client's lead: What has sustained you? What does your community value? What resources exist within your relationships and traditions? That orientation actively resists the imposition of external norms, which is a foundational concern in both cultural competence and anti-oppressive practice.
In 2022, social work education renewed its emphasis on cultural humility as a companion to cultural competence, a shift that reinforces the strengths perspective's demand for ongoing self-reflection and deference to client expertise rather than assumed professional authority.1
Indigenous and Afrocentric Adaptations
Several culturally specific frameworks have extended strengths-based thinking into communities whose knowledge systems are often excluded from mainstream practice models.
- Two-Eyed Seeing (Etuaptmumk): This Indigenous framework holds that practitioners should look with one eye through Indigenous knowledge and with the other through Western knowledge, drawing on the strengths of both without subordinating either.2 It offers a practical structure for centering Indigenous concepts of resilience, land, and community alongside conventional clinical tools.
- Whānau Ora: Developed within Māori practice, this approach treats the extended family unit (whānau) as the primary recipient of support, recognizing collective wellbeing as inseparable from individual health.2 It reframes assessment entirely around relational and community strengths.
- Afrocentric strengths model: Scholar Jerome Schiele has argued that social work must engage Afrocentric values, including communalism, spirituality, and collective identity, as genuine assets rather than cultural footnotes.2 His work challenges practitioners to reconceptualize what counts as a strength when working with African American clients and communities.
The Continuous Improvement Cultural Responsiveness Tools (CICRT), published in 2023, offer practitioners a reflexive, accountability-centered process for evaluating how well their practice actually centers the communities they serve, with particular attention to Indigenous accountability.3
The Risk of Structural Blindness
Here the perspective faces a genuine tension. Focusing on individual or community resilience can, if handled carelessly, slide into a narrative that attributes poor outcomes to insufficient personal strength rather than to structural barriers. A practitioner who celebrates a client's resilience without naming the housing discrimination, underfunded schools, or racialized policing that created the hardship is practicing something closer to victim-affirmation than anti-oppressive work.
Recent literature from 2023 and 2024 is explicit on this point: strengths-based practice must address structural inequities, not simply document assets.2 Cultural responsiveness is hollow when it stops at recognizing individual resourcefulness. Naming oppression is itself a form of honoring a client's reality.4
Practitioners seeking a broader grounding in the theoretical landscape that connects strengths-based work to anti-oppressive and critical frameworks can compare social work practice models across the major theoretical traditions.
Criticisms and Limitations of the Strengths-Based Approach
What are the criticisms of the strengths-based perspective, and do they undermine its usefulness in social work practice? This question matters because the model has become so influential that practitioners need to understand both its merits and its genuine blind spots before applying it in high-stakes settings.
Key Strengths of the Approach
Before examining criticisms, it helps to understand why the strengths perspective has gained such traction. Practitioners consistently cite several benefits:
- Client empowerment: By centering what people can do rather than what they cannot, the approach builds self-efficacy and motivation for change.
- Improved therapeutic alliance: Clients who feel seen as competent human beings rather than bundles of problems tend to engage more deeply with services.
- Cultural flexibility: The model invites practitioners to discover what each client and community values, making it adaptable across diverse populations.
- Alignment with social work values: Self-determination, dignity, and social justice are core to the profession, and strengths-based language operationalizes those ideals.
- Growing evidence base: Emerging research in areas such as mental health recovery and school social work shows promising outcomes, though more rigorous studies are needed.
Criticisms and Limitations
Scholars have raised pointed concerns that practitioners must take seriously.
- Conceptual vagueness: Gray (2011) argued that the model is "conceptually thin and empirically underdeveloped."1 Without a clear, measurable definition of "strengths," different practitioners may interpret the term in incompatible ways, making research replication difficult.
- Risk of minimizing real danger: In child protection and forensic settings, focusing on family strengths can distract from evidence of abuse, neglect, or imminent harm. Critics worry that naive optimism may endanger vulnerable clients.
- Tension with mandated reporting and risk assessment: Statutory social workers must assess danger and, at times, act coercively. An exclusive emphasis on strengths can sit uncomfortably beside these obligations, creating ethical considerations in social work.
- Lack of robust randomized controlled trial evidence: While qualitative and pilot studies are encouraging, large-scale RCTs remain scarce. This gap leaves practitioners without the level of evidence required by many funders and policymakers.
- Potential for naive optimism: Healy (2014) cautioned that highlighting resilience without addressing structural barriers can inadvertently blame clients for failing to overcome systemic disadvantage.
Counterarguments From Practitioners
Proponents respond that strengths focus does not mean ignoring problems; a well-implemented approach includes risk assessment alongside asset identification.2 Rather than replacing safety protocols, the strengths lens complements them by engaging families more effectively in safety planning. Practitioners also note that social work ethics already require balanced assessment, so the model itself is not at fault when workers misapply it. Finally, advocates call for more research funding rather than abandonment of the approach, arguing that conceptual refinement and empirical testing can address current weaknesses.
Ethical Tensions in Statutory Settings
The friction between strengths-based practice and statutory responsibilities deserves special attention. Child welfare workers, probation officers, and involuntary mental health evaluators hold legal authority that can override client self-determination. Using a strengths lens in these contexts requires transparent honesty: practitioners must acknowledge the power differential, clearly explain reporting obligations, and document risk factors even while exploring client capacities. When done skillfully, this integration can actually improve outcomes by building enough trust that clients participate in safety planning rather than hiding information.
Relevance to the ASWB Licensing Exam and MSW Curriculum
Mastering the strengths-based perspective requires balancing conceptual understanding with practical application, and nowhere is this balance more critical than when preparing for the ASWB licensing exam. The concept appears across multiple content areas, making it one of the frameworks you should know thoroughly rather than superficially.
Where Strengths-Based Content Appears on the Exam
The ASWB exam content outlines position strengths-based perspective in several locations. In exam blueprints through 2024, it appears under Content Area I: Human Development, Diversity, and Behavior in the Environment, specifically within the Human Growth and Development competency as part of "strengths-based and resilience theories."1 The 2024/2026 blueprint shifts some emphasis, placing strengths-based approaches under Content Area III: Intervention and Practice as applied knowledge.2 This dual placement reflects how exam writers view the perspective: both as a theoretical lens for understanding clients and as a practical tool for assessment and intervention.
Expect questions that test your ability to distinguish strengths-based responses from deficit-focused alternatives. Consider these sample question stems:
- A social worker is conducting an initial assessment with a client recently released from incarceration. Which approach BEST reflects the strengths perspective?
- During a family session, a mother focuses exclusively on her adolescent's behavioral problems at school. What strengths-based response would be MOST appropriate?
- A client struggling with substance use describes maintaining employment throughout their addiction. How should the social worker incorporate this information?
In each case, correct answers emphasize client assets, resilience, and self-determination rather than pathology or professional expertise.
CSWE Competency Alignment
MSW curricula integrate strengths-based practice through the Council on Social Work Education's 2022 Educational Policy and Accreditation Standards. Two competencies align directly:
- Competency 7 (Assessment): Requires social workers to collect and organize data while recognizing client strengths alongside challenges.
- Competency 8 (Intervention): Emphasizes interventions that build on identified strengths and involve clients as active partners.
Your coursework in assessment and practice classes likely reinforces these connections, even when instructors do not explicitly label activities as "strengths-based."
Exam Study Strategies
Commit the six core principles to memory. When facing multiple-choice questions, use them as a filter: does the answer option affirm client capacity, focus on possibilities, or position the client as the expert in their own life? If yes, it likely reflects the strengths perspective. Does it emphasize deficits, position the social worker as the sole expert, or focus narrowly on problems? That response probably represents a distractor rooted in deficit thinking.
Practice distinguishing language. Strengths-based answers use words like "resources," "capacities," "resilience," and "collaboration." Deficit-based distractors often emphasize "dysfunction," "disorder," "compliance," or professional authority. This linguistic sensitivity helps you quickly narrow choices under timed conditions. Pairing this approach with a structured ASWB exam prep course can sharpen your timing and confidence across all content areas.
Frequently Asked Questions About the Strengths-Based Perspective
Below are answers to the most common questions prospective and current social workers ask about the strengths-based perspective. Each answer offers a concise overview; see the referenced sections of this article for a deeper discussion.
Explore More
- Attachment Theory in Social Work
- Ecological Systems Theory in Social Work
- Erikson's Psychosocial Development Theory in Social Work
- Psychodynamic Theory in Social Work
- Rational Choice Theory in Social Work
- Social Exchange Theory in Social Work
- Social Learning Theory in Social Work
- Systems Theory in Social Work