Points of interest…
- Psychodynamic theory adapts Freud's ideas into four distinct schools: drive theory, ego psychology, object relations, and self psychology.
- Brief psychodynamic models fit agency-based practice into 8 to 16 sessions, countering the myth that this approach requires years.
- A 2010 meta-analysis reported a 1.51 effect size at long-term follow-up, showing client gains often strengthen after therapy ends.
- Defense mechanisms and transference appear in roughly 12 percent of licensed clinical social work exam questions on the ASWB.
Roughly 12 percent of licensed clinical social work exam items test defense mechanisms and transference phenomena, placing psychodynamic concepts among the most exam-critical material in the ASWB blueprint. Social workers encounter the same dynamics daily when clients repeat destructive relationship patterns or act in ways that baffle their conscious intentions. Psychodynamic theory provides a language for naming these unconscious processes and for working with them rather than around them.
Unlike intensive psychoanalysis, which demands multiple sessions per week over years, psychodynamic thinking now shapes brief, evidence-supported interventions used in hospitals, schools, and child welfare agencies. It has moved well beyond the couch.
Mastering this framework is not just about passing the licensing exam. It is about recognizing when a client's anger in a child welfare conference is really terror from an old trauma, and responding to the person, not just the behavior. For a broader view of how psychodynamic thinking fits alongside other social work theories and practice models, the theories hub situates this framework within the full landscape of approaches social workers draw on every day.
What Is Psychodynamic Theory? How It Differs From Psychoanalysis
Classical psychoanalysis involves a patient lying on a couch, free-associating four or five days a week, often for years, while an analyst sits out of view and interprets unconscious conflicts rooted in early childhood. Psychodynamic theory, by contrast, is an umbrella framework that draws on psychoanalytic concepts: unconscious processes, defense mechanisms, and the influence of early attachment. It adapts them for broader clinical settings, shorter treatment windows, and integration with environmental, systemic, and here-and-now interventions. For social workers, this distinction is fundamental: psychodynamic social work practice borrows the lens of internal emotional life but reshapes it to fit schools, hospitals, foster care agencies, and community clinics where long-term, high-frequency therapy is neither feasible nor appropriate.
Early Adoption by the Social Work Profession
Social work embraced psychodynamic thinking earlier than most helping professions. Mary Richmond's pioneering work in the 1920s intersected with the rise of psychiatry, and by the 1930s the diagnostic school at Smith College School for Social Work had fully incorporated Freudian concepts into casework training. Unlike psychiatry or psychology, however, social work never fully adopted orthodox psychoanalysis. The profession's commitment to person-in-environment fit and its presence in public agencies, settlement houses, and child welfare settings demanded a more flexible, eclectic approach. As a result, psychodynamic social work evolved into a distinct practice model that retained attention to transference, defense mechanisms, and unconscious motivation while incorporating systems theory in social work, family dynamics, and advocacy.
Four Key Markers That Distinguish Psychodynamic Social Work from Psychoanalysis
- Shorter duration: Psychodynamic social work typically unfolds over weeks or months, not years, and may take the form of brief psychodynamic therapy lasting twelve to twenty sessions.
- Focus on here-and-now functioning: While early experience is acknowledged, the primary goal is improving current relationships, symptoms, and social roles, not exhaustive reconstruction of childhood.
- Attention to environment and systems: Practitioners assess housing, income, racism, school climate, and family structure alongside intrapsychic dynamics, and they intervene at multiple levels.
- Use in non-clinical settings: Psychodynamic assessment informs child-welfare permanency planning, discharge planning in medical social work, school crisis intervention, and supervision, not only outpatient therapy.
What Is the Difference Between Psychoanalytic and Psychodynamic Theory in Social Work?
Psychoanalytic theory refers to the original body of work by Freud and his immediate followers, centered on drive theory, the structural model (id, ego, superego), and intensive treatment. Psychodynamic theory is the broader, evolving family of approaches, including ego psychology, object relations, self psychology, and relational psychoanalysis, that social work theories and practice models draw on selectively. In social work, psychodynamic theory functions as a clinical lens, not a singular treatment protocol, and it is almost always integrated with other frameworks such as cognitive-behavioral, trauma-informed, or strengths-based practice.
Origins and Key Theorists: From Freud to Self Psychology
Psychodynamic theory is not one theory but four overlapping schools, each one redirecting what social workers listen for in a session. Most explainers list the names without explaining the shift each school produced. The distinctions matter because they change your assessment focus, your interventions, and what you document as clinically significant.
Freud and Drive Theory
Sigmund Freud (1856 to 1939) proposed that behavior is driven by unconscious sexual and aggressive impulses, organized through the structural model of id, ego, and superego. For social workers, the lasting contribution is the premise that clients act on motives they cannot fully articulate, which is why presenting problems rarely match underlying conflicts. Freudian theory trains practitioners to take symptoms seriously as communication rather than as the whole story.
Ego Psychology
Anna Freud, Heinz Hartmann, and Erik Erikson moved attention away from drives and toward the ego's capacity to cope, adapt, and master developmental tasks. Hartmann argued the ego has conflict-free zones (memory, perception, motor control) that support healthy functioning, while Erikson mapped psychosocial stages across the lifespan , work explored in depth through Erikson's psychosocial development theory in social work. This school shaped social work's enduring focus on adaptive functioning, strengths, and person-in-environment assessment. When you evaluate a client's coping skills, frustration tolerance, or reality testing, you are using ego psychology.
Object Relations
Melanie Klein, D.W. Winnicott, and Ronald Fairbairn shifted the lens from instincts to relationships, arguing that early caregiver bonds become internalized templates ('internal objects') that shape every later relationship. For social work, this school explains why a client repeats destructive partnerships, mistrusts helpers, or recreates childhood dynamics with a caseworker. It tells you to pay attention to relational patterns, not just symptoms.
Self Psychology
Heinz Kohut centered the development of a cohesive self through empathic attunement from caregivers (whom he called 'selfobjects'). When attunement fails, the self fragments and clients seek mirroring, idealization, or twinship in later relationships. For social workers, self psychology validated empathy as a clinical intervention, not just a rapport-building stance. It also reframed narcissistic injury and shame as developmental wounds rather than character flaws.
Attachment Theory as a Psychodynamic Offshoot
John Bowlby integrated psychoanalytic thinking with ethology and developmental research to produce attachment theory in social work, identifying secure, anxious, avoidant, and disorganized patterns rooted in early caregiver responsiveness. Child welfare practice relies on attachment frameworks heavily: removal decisions, reunification planning, foster placement matching, and trauma-informed parenting interventions all draw on Bowlby's work and its extensions by Mary Ainsworth and Mary Main.
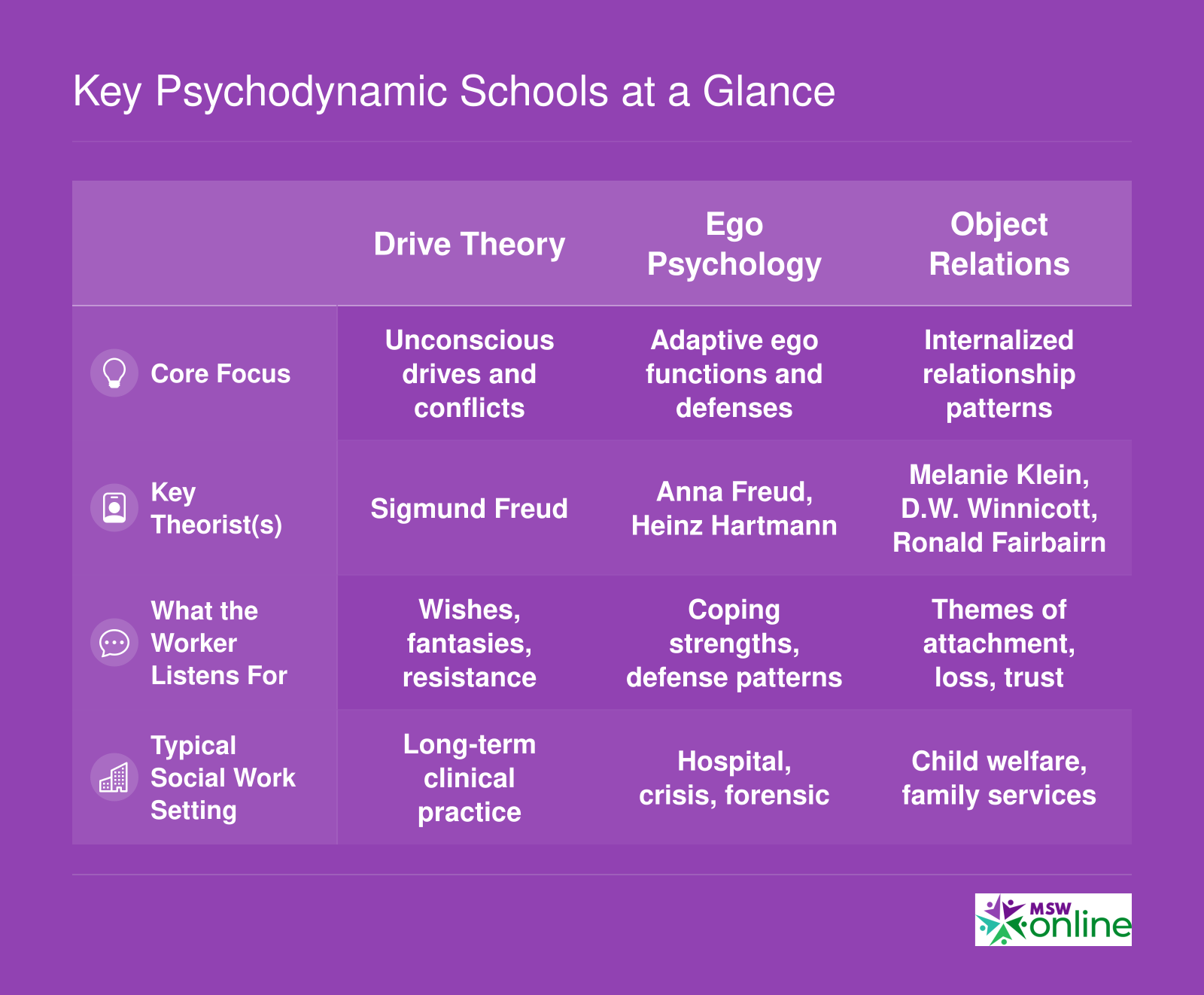
Key Psychodynamic Schools at a Glance
Students often encounter these schools in textbooks as overlapping walls of text. The table below isolates what matters for social work practice: the core focus each school brings, whose work you should know, what to listen for in sessions, and where you are most likely to use it.
Core Concepts and Key Terms Every Social Worker Should Know
The Association of Social Work Boards lists defense mechanisms and transference phenomena in roughly 12 percent of licensed clinical social work exam questions, making these concepts both clinically essential and exam-critical. Psychodynamic theory introduces a vocabulary that helps social workers name and understand patterns they see every day in supervision, in client interviews, and in their own emotional reactions.
Unconscious Processes
Psychodynamic theory rests on the premise that much of human motivation, memory, and emotion operates below conscious awareness. A foster youth who says he does not care about reunification but sabotages every permanency plan may be acting on unconscious fear and grief. Social workers trained in this lens listen for contradictions between stated goals and actual behavior, using them as diagnostic clues rather than dismissing clients as unmotivated.
Defense Mechanisms
Defense mechanisms are unconscious strategies the ego uses to manage anxiety and protect self-esteem. Social workers encounter them in nearly every practice setting. Common mechanisms include denial (a parent insists there is no domestic violence despite police records), projection (a client accuses the social worker of being angry when the client himself is furious), splitting (a teen labels staff as all-good or all-bad with no middle ground), rationalization (a client explains away a relapse with logical-sounding excuses), and sublimation (channeling anger into activism or art). Recognizing defenses allows workers to respond with empathy rather than confrontation, meeting clients where they are emotionally.
Transference and Countertransference
Transference occurs when a client unconsciously redirects feelings about significant past relationships onto the social worker. A middle-aged client may treat a young practitioner with the deference he showed an authoritarian father. Countertransference is the worker's emotional response to the client, shaped by the worker's own history and unresolved conflicts. A social worker who becomes overly protective of a neglected child may be reacting to her own childhood experience. These phenomena are not treatment failures but sources of insight. Supervision routinely explores countertransference to prevent bias and burnout.
Resistance
Resistance describes any behavior that impedes therapeutic progress: missed appointments, sudden topic changes, or intellectualizing painful emotions. Psychodynamic workers interpret resistance as protective rather than defiant, exploring what the client fears will happen if change proceeds.
The Structural Model: Id, Ego, and Superego
Freud's structural model divides the psyche into three systems. The id holds unconscious drives and wishes, the superego houses internalized moral rules and parental standards, and the ego mediates between the two while managing reality. A client paralyzed by guilt (overactive superego) or one who acts impulsively without regard for consequences (weak ego) illustrates this framework in action.
Attachment Styles
Though rooted in developmental psychology, attachment theory stages have become central to contemporary psychodynamic social work. Secure, anxious-ambivalent, avoidant, and disorganized attachment styles shape how clients form relationships, tolerate intimacy, and engage in treatment. A client with disorganized attachment may oscillate between clinging and hostility, confusing workers unfamiliar with the pattern.
What Are the 5 Stages of Psychodynamic Theory?
This common search query reflects confusion: psychodynamic theory does not have a single canonical five-stage model. The question likely refers to Freud's five psychosexual stages (oral, anal, phallic, latency, genital) or Erikson's stages of psychosocial development. Freud's stages appear occasionally on licensing exams as historical context; Erikson's stages are tested more frequently and remain clinically relevant across the lifespan. Social workers should know both frameworks but prioritize Erikson for exam preparation and practice application.
Questions to Ask Yourself
How Social Workers Apply Psychodynamic Theory in Practice
Psychodynamic theory has moved well beyond the therapy couch and now shapes how social workers think about clients across every level of practice, from one-on-one sessions to organizational dynamics.
Micro Level: Individual Practice and the Case Vignette
At the micro level, applying psychodynamic theory means slowing down to ask why a pattern keeps repeating, not just what the client should do differently. Consider Marcus, a 26-year-old referred after losing three jobs in two years. Each termination followed a conflict with a male supervisor. In individual sessions, the social worker notices Marcus grows defensive and withdrawn whenever she raises the topic of feedback from authority figures. Rather than confronting the behavior directly, she tracks the pattern across sessions.
Over time, Marcus begins to articulate that his father was hypercritical and dismissive. The social worker recognizes that Marcus may be experiencing transference, relating to his supervisors as though they were his father, and responding with the same protective withdrawal he learned as a child. She names this pattern carefully: "I notice that when we talk about your boss's comment, you pull back the same way you described doing with your dad."
This is psychodynamic theory in action at the micro level. The concrete clinical actions are:
- Observation: Track recurring relational themes across sessions, not just presenting problems.
- Reflection: Use open-ended questions to connect present patterns to earlier experiences.
- Interpretation: Offer tentative connections between past relationships and current behavior, checking the client's response.
- Countertransference monitoring: Notice your own emotional reactions to the client as data about the therapeutic relationship.
Marcus gradually begins to distinguish his supervisors from his father, reducing the automatic defensive reaction that had been costing him jobs.
Mezzo Level: Group Work and Family Intervention
In group settings, psychodynamic thinking surfaces through parallel process. A supervision group that becomes unusually competitive and dismissive may be unconsciously mirroring the dynamics of a client family they are treating together. Recognizing this allows the supervisor to name what is happening and redirect the group's energy.
In family intervention, the theory draws attention to intergenerational transmission of attachment patterns. A parent who was neglected may struggle to read their infant's cues, not from indifference but from an unprocessed relational history. The social worker's role is to help the parent develop awareness of that history and interrupt the cycle, often through guided reflection on their own childhood experiences alongside observation of the current parent-child interaction.
Macro Level: Organizations and Community Trauma
At the macro level, psychodynamic concepts help explain why institutions resist change even when change is clearly needed. An organization may collectively deny the severity of a systemic problem, deploying what amounts to institutional defense mechanisms that protect staff from uncomfortable truths. Community-level trauma, such as the lingering effects of historical displacement or chronic disinvestment, can also be understood through a psychodynamic lens that attends to collective grief, silenced narratives, and cycles of helplessness passed across generations. The application here is interpretive rather than clinical, and social workers use it to inform advocacy and organizational consultation rather than direct treatment.
Across all three micro, mezzo, and macro levels of social work, the answer to how to use psychodynamic theory in practice is consistent: use it to look beneath the surface behavior, trace relational patterns to their origins, and intervene at the point where insight can interrupt repetition.
Psychodynamic Assessment in Child Welfare, Hospital, and School Settings
Psychodynamic assessment is the art of listening beneath the presenting problem to uncover the unconscious conflicts and relational patterns that drive a client's distress. Unlike a standard diagnostic interview, this approach treats the assessment itself as a reflective space where hidden themes emerge through what is said, omitted, repeated, or avoided. Social workers in child welfare, hospitals, and schools use this lens to move from a surface-level problem to a deep understanding of the person and their inner world, leading to interventions that actually stick.
The Three Components of Psychodynamic Assessment
The process unfolds in three overlapping phases, each demanding active curiosity rather than a checklist.
- Intake: Listening for Unconscious Themes , Beyond gathering demographic and presenting data, the worker tunes into emotional tone, contradictions, and narrative patterns. A parent might describe a child's aggression while unconsciously minimizing their own fear of losing control. The worker notes these cues without immediate interpretation.
- Case Formulation: Linking the Present to the Past , The core task is to connect current symptoms to early relational templates, core conflicts, and characteristic defenses. The formulation answers "Why does this person struggle in this way at this time?" by tracing the problem to its developmental roots. It identifies the client's dominant object relations, ego strengths, and attachment style.
- Treatment Planning: Matching Interventions to Ego Strength , Recommendations flow directly from the formulation. A client with fragile ego boundaries may first need supportive techniques to build trust before any exploratory work. For someone with good insight and observing ego, brief dynamic therapy can target a specific relational pattern. The plan is not a one-size protocol but a tailored map of what to address, in what order, and at what depth.
Applying the Framework in Child Welfare: A Foster Child's Attachment Disruption
Consider Maya, age 7, removed from a neglectful home and placed with a foster family. She refuses to speak to adults, hoards food, and punches other children. A DSM diagnosis might note oppositional defiant disorder or reactive attachment disorder. A psychodynamic assessment goes further. The intake reveals that Maya's birth mother often forgot to feed her and would disappear for days. The worker's quiet, consistent presence during the interview begins to evoke Maya's deep fear of being forgotten again. Case formulation frames her hoarding as a survival defense against literal starvation, and her aggression as a reenactment of the angry-abandonment cycle she internalized. She pushes adults away before they can leave her. Based on this attachment theory in social work understanding, treatment planning prioritizes creating a predictable, emotionally attuned foster environment where Maya can internalize a new, safer object. Interpretations about her anger wait until she develops enough trust to use them.
Medical Social Work: Understanding Non-Adherence Through Defense Mechanisms
In a hospital, Mr. Alvarez, a 58-year-old with diabetes, repeatedly misses appointments and ignores his insulin regimen despite understanding the medical consequences. Medical staff label him non-compliant. A psychodynamic assessment begins by sitting with him and listening. The intake uncovers that his father died of diabetes complications when Mr. Alvarez was a teenager, and that he experiences his own diagnosis as a shameful repetition. Case formulation identifies denial and intellectualization as key defenses: he can rattle off diabetic facts while emotionally disconnecting from his body. Underneath, he is terrified of becoming like his father. The formulation links his current non-adherence to an unconscious fantasy that if he refuses the sick role, he can escape his father's fate. Treatment planning thus shifts from education to exploring his grief and reframing self-care as an act of strength, not a submission to illness. The social work role in healthcare team is advised to avoid power struggles and instead validate his loss.
School Social Work: Acting-Out as Communication
In a school setting, a fourth-grader's disruptive behavior often signals unmet relational needs. A boy who constantly provokes his teacher may be reenacting a chaotic home environment where attention comes only through conflict. Psychodynamic assessment helps the school social worker see the behavior as a communication: "Notice me, contain me, show me I exist." The formulation might identify a fundamental deficit in self-esteem regulation because early caregivers were consistently dismissive. The intervention becomes about providing a stable, caring relationship within the school day rather than merely enforcing behavioral consequences.
Beyond the DSM: The Psychodynamic Formulation
Standard diagnostic systems describe symptom clusters. A psychodynamic formulation answers the deeper questions: Why this symptom? Why now? Why this person? It explains the meaning of the symptom within the client's life history and current relational field. For Maya, food hoarding is not just a behavioral problem but a symbol of early starvation and object loss. For Mr. Alvarez, non-adherence is an attempt to ward off terrifying identification with a dead parent. This understanding guides interventions that heal rather than simply manage, making psychodynamic assessment an indispensable tool across all social work settings.
Brief Psychodynamic Models for Agency-Based and Time-Limited Practice
A common objection to psychodynamic work is that it requires years on the couch. That stereotype no longer reflects the field. Several structured brief models translate psychodynamic principles into the 8 to 16 session windows that managed care, mandated services, and high-volume agencies actually allow.
Four Brief Models Worth Knowing
- Short-Term Psychodynamic Psychotherapy (STPP): Typically delivered in 12 to 25 sessions, with adapted protocols running as short as 6 to 12 sessions.1 The therapist identifies a focal conflict early and works it consistently across the engagement. STPP has the strongest evidence base of the brief models, with research support for depression, anxiety disorders, and some personality disorders.2
- Luborsky's Supportive-Expressive Therapy (SET): Usually 16 to 40 sessions, with brief applications of 6 to 8 sessions.3 SET is organized around the Core Conflictual Relationship Theme (CCRT), a structured way to map a client's recurring wish, the response from others, and the response of the self.3 The CCRT gives the worker a one-page formulation to guide every session.
- Intensive Short-Term Dynamic Psychotherapy (ISTDP) and Davanloo's model: Both run 20 to 40 sessions and use active techniques to surface defenses and unconscious feelings quickly.2 Malan's Short-Term Dynamic Psychotherapy, a related approach, is structured around roughly 20 sessions.4
- Mann's Time-Limited Psychotherapy and Dynamic Interpersonal Therapy (DIT): Mann's model uses a strict 12-session frame, with the termination theme introduced around session 6 and four sessions dedicated explicitly to ending.4 DIT is a manualized 16-session model originally developed for depression in public mental health systems.3
How Brief Models Fit Agency Realities
Agency caseloads rarely permit open-ended exploration. Brief psychodynamic models adapt by front-loading the formulation. By the second or third session, the worker names a focal dynamic (often a relational pattern, an unresolved loss, or a defense that drives the presenting problem) and contracts explicitly with the client around it. Sessions then return to that focus rather than chasing weekly crises.
This structure also fits mandated clients and managed care authorization cycles. A documented focal formulation justifies medical necessity, supports reauthorization requests, and gives supervisors something concrete to review. For practitioners who want to situate these models within a broader framework, the strengths-based perspective in social work offers a complementary lens that pairs well with psychodynamic formulation in agency settings.
A Six-Session Example
Even a 6-session intervention can be psychodynamic if the formulation is sharp. Imagine a client referred after a workplace conflict. Sessions one and two map the CCRT: a wish to be respected, an expected dismissal from authority figures, and a self-response of withdrawal. Sessions three through five test that pattern against current relationships and the working alliance itself. Session six addresses termination as a live example of the pattern. The work is short, but it is not shallow.
What the Evidence Says: Research Support for Psychodynamic Social Work
A 2010 meta-analytic review published in American Psychologist reported that short-term psychodynamic psychotherapy produced effect sizes of 0.97 immediately post-treatment and 1.51 at long-term follow-up, demonstrating that gains often strengthen after therapy ends.1 These numbers place psychodynamic interventions in the large-effect range by conventional standards and suggest durability that compares favorably to many evidence-based treatments.
Comparative Outcomes Across Disorders
Meta-analyses consistently show psychodynamic therapy achieving comparable outcomes to cognitive-behavioral therapy for depression and anxiety. For depression, post-treatment effect sizes average around 0.69 to 0.81, rising to 1.29 at follow-up.1 Anxiety outcomes are equally robust, with post-treatment effects near 1.08 and follow-up effects reaching 1.35.1 A 2004 meta-analysis by Leichsenring, Rabung, and Leibing found within-group effect sizes of 1.39 post-treatment and 1.57 at follow-up for short-term psychodynamic therapy delivered in an average of 21 sessions.1 For personality disorders, long-term psychodynamic psychotherapy demonstrated an effect size of 1.46 at follow-up in the 2010 review, a finding echoed in Leichsenring and Rabung's 2008 analysis of 23 studies.2 These effect sizes are not smaller than those reported for other evidence-based modalities and in some cases exceed them at long-term measurement points.
The Evidence Gap for Social Work Delivery
Most randomized controlled trials of psychodynamic therapy enroll psychologists or psychiatrists as treating clinicians, not licensed social workers. Few studies isolate the contribution of provider discipline, making it difficult to assert that the same outcomes transfer when a social worker delivers the intervention in a community mental health center or child welfare setting. Meta-analyses by Abbass and colleagues examining intensive short-term dynamic psychotherapy report effect sizes between 0.7 and 1.3, but the clinician samples are heterogeneous and rarely specify social work degrees.3 This gap does not mean psychodynamic concepts are ineffective when social workers use them; it means the evidence base specific to social work practice remains thinner than the broader literature. Social work research and practice offers additional context for understanding how evidence hierarchies shape clinical decision-making in the field.
Real-World Integration and the Research Lag
The evidence base for psychodynamic therapy is growing but still lags behind cognitive-behavioral approaches in volume and specificity. Cochrane reviews and NICE guidelines often rank psychodynamic interventions as supported but less extensively tested, particularly for specific diagnoses and populations.4 As a result, most social workers integrate psychodynamic concepts into eclectic practice rather than delivering manualized psychodynamic therapy as a standalone protocol. Understanding transference, defense mechanisms, and attachment dynamics enriches case formulation and rapport building even when the formal treatment plan includes cognitive restructuring or solution-focused techniques. The research supports the value of psychodynamic thinking; it simply does not yet prescribe it as the exclusive or universally first-line approach across all settings.
A 2010 meta-analysis published in American Psychologist found that psychodynamic therapy patients continued to improve after treatment ended, achieving a large effect size of 1.51 at long-term follow-up. In contrast, gains from some short-term therapies tended to plateau or decline once sessions stopped, suggesting psychodynamic work may catalyze sustained growth.
Strengths, Criticisms, and Cultural Considerations
Psychodynamic theory remains one of the most widely taught frameworks in social work education, yet it carries real limitations that practitioners must weigh honestly. The lists below summarize the major advantages and drawbacks, followed by a closer look at cultural considerations every social worker should keep in mind.
Pros
- Offers deep insight into unconscious motivations and relational patterns that surface-level models often miss entirely.
- Places the therapeutic alliance at the center of change, strengthening engagement across micro and mezzo settings.
- Explains repetitive, 'stuck' behavioral patterns by tracing them to early relational experiences and unresolved conflicts.
- Adapts well across practice contexts, from child welfare to medical social work to private clinical practice.
- Complements trauma-informed care by illuminating how defense mechanisms and attachment disruptions shape a client's present functioning.
- Provides a rich language for supervision and reflective practice, helping workers examine their own emotional responses to clients.
Cons
- Rooted in Eurocentric assumptions that historically centered white, middle-class, Western family structures as normative.
- Foundational research drew on narrow, non-diverse samples, limiting generalizability to many populations social workers serve.
- Traditional models require long-term, frequent sessions that conflict with agency time limits and managed-care realities.
- Outcomes are difficult to measure with standardized tools, creating tension with evidence-based practice mandates.
- Risks pathologizing culturally normative behaviors, such as communal decision-making or spiritual experiences, when viewed through an individualistic lens.
- Power dynamics inherent in the expert-interpreter role can replicate oppressive hierarchies, especially across lines of race, gender, or class.
- Classical psychoanalytic thought largely ignored how racism, colonialism, and systemic oppression shape the unconscious and relational life.
Psychodynamic Theory and the ASWB Licensing Exam
Memorizing definitions vs. identifying concepts in vignettes: the ASWB exam rewards the second skill, not the first. You will rarely see a question asking "What is projection?" You will frequently see a case scenario in which a client behaves in a way that illustrates projection, and you must name it.
Where Psychodynamic Content Appears on the Exam
Psychodynamic concepts sit primarily in Content Area I, Human Development, Diversity, and Behavior in the Environment, on both the ASWB Masters and Clinical exams.1 They also surface in Assessment and Intervention Planning when questions ask you to choose a treatment approach or interpret client behavior. The current content outlines (the 2018 versions) remain in effect through summer 2026, with the next outline, based on the 2024 practice analysis, launching August 3, 2026.2 If you are testing after that date, confirm the new KSAs on the ASWB site.
The Highest-Yield Concepts to Study
Both ASWB and major prep providers flag defense mechanisms as the single highest-yield psychodynamic topic.3 Prioritize:
- Defense mechanisms: Denial, projection, displacement, sublimation, reaction formation, rationalization, intellectualization, regression, repression, and splitting. Know how each looks in a clinical scenario.1
- Transference and countertransference: Recognize when a client reacts to you as if you were someone from their past, and when your own reactions signal unresolved material.
- Ego functions: Reality testing, impulse control, judgment, and defensive functioning.
- Erikson's eight psychosocial stages: Match the stage to the client's age and presenting conflict.3
- Freud's structural model (id, ego, superego) and psychosexual stages (oral, anal, phallic, latency, genital).4
- Object relations basics: Internalized representations of self and others, especially relevant to attachment and personality disorder questions.
- The distinction between psychoanalytic and psychodynamic approaches: Frequency, duration, and the role of the unconscious vs. present-day relational patterns.1
Sample Question Stems
- A client who repeatedly arrives late and avoids discussing her father is most likely demonstrating which defense mechanism? Answer: avoidance, or more precisely repression or resistance, depending on options. The clinical clue is the pairing of behavioral avoidance with a specific relational topic.
- A social worker notices she feels unusually protective of a young client who reminds her of her own daughter. This is best described as: countertransference. The marker is the worker's reaction originating in her own history.
- A 65-year-old client reviewing regrets about his career is navigating which Eriksonian stage? Integrity vs. despair. For a deeper review of each stage and how to apply it in practice, see Erikson's stages of psychosocial development in our theory resources.
Study Tip
Drill vignettes, not flashcards. Use a social work exam prep question bank, read each stem twice, and force yourself to name the concept before reading the answer choices. The exam tests recognition under clinical disguise, so train that exact skill.
If you learn only one psychodynamic concept deeply, make it countertransference. Recognizing your own emotional reactions to clients is the gateway skill for psychodynamic practice, productive supervision conversations, and ethical boundary maintenance. It is also a tested topic on the ASWB licensing exam, so mastering it serves both your clinical growth and your exam preparation.
Frequently Asked Questions About Psychodynamic Theory in Social Work
Below are answers to the questions prospective and current social workers ask most often about psychodynamic theory. Each response is intentionally concise; for deeper exploration, refer to the relevant section of this guide.
Related Articles
Explore More
- Attachment Theory in Social Work
- Ecological Systems Theory in Social Work
- Erikson's Psychosocial Development Theory in Social Work
- Rational Choice Theory in Social Work
- Social Exchange Theory in Social Work
- Social Learning Theory in Social Work
- Strengths-Based Perspective in Social Work
- Systems Theory in Social Work