Points of interest…
- Social determinants of health drive up to 80 percent of health outcomes, making social work interventions a direct lever for cutting costs.
- Integrated social work teams have reduced hospital readmission rates by 25 percent or more in documented case studies.
- Healthcare social workers can bill Medicare directly using specific CPT codes, strengthening their financial value to employers.
- BLS projects healthcare social worker employment to grow faster than average, with a national median salary near $62,000.
U.S. national health expenditures hit roughly $4.8 trillion in 2023, with CMS forecasting $7 trillion by 2031. A significant portion of that spending is linked to unaddressed social determinants, including housing instability, food insecurity, and transportation gaps, that trigger preventable hospitalizations and repeat emergency visits.
Healthcare social workers are the professionals trained to tackle those upstream drivers directly. They secure discharge placements, navigate insurance complexities, and connect patients with community resources that keep them out of hospitals. As payers shift to value-based reimbursement, embedding social workers is becoming a financial necessity, not just a clinical support.
Why U.S. Healthcare Costs Keep Rising, and Where Social Determinants Fit In
U.S. national health expenditures reached roughly $4.8 trillion in 2023, according to data published by the Centers for Medicare & Medicaid Services (CMS) on its National Health Expenditure Data page. That figure has grown at an average annual rate of roughly 4 to 5 percent in recent years, outpacing both inflation and wage growth. Yet despite spending more per capita than any other high-income nation, the United States consistently lags on key population health measures such as life expectancy, infant mortality, and chronic disease prevalence. Understanding why requires looking beyond hospital bills and prescription drug prices.
The Social Determinants Gap
Research from the National Academies of Sciences, Engineering, and Medicine (NASEM) has long emphasized that clinical care accounts for only a portion of what determines a person's health. A widely cited framework, drawing on NASEM analyses and echoed by the World Health Organization, estimates that social determinants of health (SDOH) drive as much as 80 percent of health outcomes. These determinants include:
- Housing instability: Patients without stable shelter cycle through emergency departments at far higher rates.
- Food insecurity: Nutritional deficits worsen diabetes, heart disease, and other chronic conditions.
- Transportation barriers: Missed appointments and delayed care lead to costly acute episodes.
- Social isolation: Loneliness correlates with higher rates of hospitalization, especially among older adults. Evidence-based strategies for combating loneliness in older adults show promise in reducing these preventable admissions.
- Economic hardship: Inability to afford medications or copays drives non-adherence, which in turn drives readmissions.
Kaiser Family Foundation analyses reinforce the point: states that invest less in social services relative to healthcare tend to see worse health outcomes and higher per-capita spending.
Why Traditional Spending Alone Cannot Solve the Problem
Most healthcare dollars flow to treatment after a condition has already become acute. Hospital stays, surgeries, and specialty drugs consume the largest share of national health expenditures. Meanwhile, upstream factors like poverty, education gaps, and unsafe housing remain largely outside the clinical reimbursement model. Peer-reviewed literature available through PubMed consistently demonstrates that addressing SDOH before patients reach a crisis can reduce emergency department visits, shorten inpatient stays, and lower 30-day readmission rates.
This is exactly the gap social workers are trained to fill. With expertise in psychosocial assessment, community resource navigation, and behavioral health intervention, healthcare social workers target the non-clinical drivers that inflate costs. The sections that follow break down how those interventions translate into measurable savings across hospital, primary care, and community settings.
What Do Social Workers Do in Healthcare Settings?
Clinical teams solve medical problems. Social workers solve the problems that determine whether the medical solution actually works.
Core Daily Functions
In any given shift, a healthcare social worker moves across a wide range of tasks that rarely get captured in a billing code but consistently shape patient outcomes. Those tasks typically include:
- Psychosocial assessments: Evaluating a patient's mental health, family dynamics, housing situation, and financial stressors that affect recovery.
- Discharge planning: Coordinating the transition from hospital to home, skilled nursing, or rehabilitation, identifying what the patient needs and who will provide it.
- Care coordination: Communicating across physicians, nurses, case managers, insurers, and community agencies so no part of the plan falls through the gaps.
- Crisis intervention: Responding to suicidal ideation, domestic violence disclosures, or acute psychiatric episodes within the clinical setting.
- Advance-care-planning conversations: Helping patients and families articulate goals of care, understand prognosis, and document their wishes before a crisis forces the decision.
The Bridge Role
A physician can write a discharge order in two minutes. Turning that order into something a patient can actually follow may take hours of social work. That gap is where readmissions happen.
The social worker translates clinical language into actionable steps: scheduling the follow-up appointment, confirming the patient has transportation to get there, connecting them with a medication assistance program if cost is a barrier, and looping in a home health agency if mobility is limited. Without that translation work, even a medically sound discharge plan can collapse within 72 hours.
On interdisciplinary rounds, the social worker is often the first person to surface information the rest of the team does not have. A patient refusing discharge may not be difficult; they may have no one at home to help them and no way to say so directly. That insight, surfaced early, changes the plan and prevents a costly return visit.
Settings Where Social Workers Practice
Healthcare social workers operate across a broader range of environments than most people realize:
- Hospitals: Inpatient units, emergency departments, and trauma centers.
- Primary care clinics: Embedded roles focused on behavioral health integration and chronic disease management.
- Hospice and palliative care: Guiding families through end-of-life decisions and grief support. If this area interests you, learn more about how to become a hospice social worker.
- Managed care organizations: Utilization review, member outreach, and high-risk population management.
- Outpatient behavioral health: Therapy, case management, and linkage to community supports. Those drawn to crisis-focused clinical work may also consider a path as a psychiatric social worker.
Across all of these settings, the common thread is the same: social workers see the full picture of a patient's life, not just the presenting diagnosis.
Questions to Ask Yourself
How Social Work Interventions Reduce Costs: The Evidence
A growing body of research confirms that social work interventions deliver measurable savings across healthcare systems. Understanding these findings can help administrators, policymakers, and practitioners make the case for expanding social work's role in clinical settings.
A systematic review of 16 studies published in the American Journal of Public Health found consistent evidence that social work services lower costs at multiple points along the care continuum.1 Three intervention areas stand out.
Discharge planning. Social workers who coordinate discharge plans help patients transition safely from hospital to home or community-based care. Studies show these efforts reduce hospital readmissions by 15 to 30 percent and shorten the average length of stay by 0.5 to 2 days, translating to savings of $200 to $1,000 per patient.1
Super-utilizer programs. A small share of patients accounts for a disproportionate share of healthcare spending, with annual acute care costs ranging from $20,000 to $50,000 per person.2 Social workers embedded in super-utilizer programs connect these patients to housing, behavioral health, and food insecurity screening tools so that underlying needs are addressed before they escalate. The result is a 10 to 30 percent reduction in emergency department visits, or roughly 0.5 to 2 fewer visits per patient.2
Care coordination for high-need Medicaid enrollees. In a trial of 240 patients, a social worker-led care coordination model demonstrated that sustained, relationship-based case management can redirect spending from costly acute episodes toward preventive and community services.3 Professionals interested in leading this type of research may consider a career as a research social worker.
Across these intervention types, economic analyses report a return on investment ranging from 1.5 to 4.0 dollars for every dollar spent on social work services.2 The evidence is clear: investing in social work is not simply a matter of compassion but a financially sound strategy for healthcare organizations aiming to control costs while improving patient outcomes. For practitioners who want to deepen their clinical expertise, pursuing a clinical social work MSW can open doors to leadership roles in these high-impact programs.
The Cost Impact of Social Work at a Glance
Across hospital systems, clinics, and community health programs, social work interventions consistently produce measurable savings. The figures below summarize the strongest evidence on how embedding social workers into care teams drives down costs.

Social Workers and Healthcare Reimbursement Navigation
Can clinical social workers bill Medicare directly, and which CPT codes actually apply to social work services?
Those are not abstract questions for a social worker in a hospital or outpatient setting. Reimbursement recognition shapes what services get delivered, how departments justify headcount, and whether preventive or transitional care actually happens at scale. Understanding the billing landscape is part of practicing effectively in healthcare.
LCSWs as Medicare Part B Providers
Licensed Clinical Social Workers are recognized as independent providers under Medicare Part B. The authoritative source for how this recognition works, what services are covered, and what conditions apply is the CMS Medicare Benefit Policy Manual, Chapter 15. That chapter specifies covered outpatient mental health services, provider qualifications, and documentation requirements. Before billing Medicare under your own NPI, read Chapter 15 directly rather than relying on secondhand summaries, because scope and documentation standards matter for audit purposes.
State Medicaid programs operate on separate rules. Whether an LCSW can bill Medicaid, and for which services, varies by state. Each state publishes its own Medicaid provider manual, and that manual is the definitive resource. Do not assume that Medicare billing recognition transfers automatically to your state's Medicaid program. Note that billing eligibility is tied to specific levels of social work licensure, so confirming your credential level is a necessary first step.
CPT Codes Relevant to Social Work Practice
Several code families appear regularly in social work billing contexts, though coverage and reimbursement rates depend on payer, setting, and your specific licensure:
- Health and Behavior Assessment/Intervention (96150-96155): These codes cover psychological and behavioral assessment and intervention for patients with physical health conditions, distinct from mental health diagnoses.
- Transitional Care Management (99495-99496): These codes reimburse care coordination services during the high-risk period following a hospital or facility discharge. Social workers who coordinate post-discharge planning frequently contribute to the work captured under these codes, though billing attribution depends on how the practice is structured.
- Chronic Care Management (99490): This code applies to non-face-to-face care coordination services for patients with two or more chronic conditions. Social workers embedded in primary care or integrated care teams may contribute substantially to the activities this code covers.
For current reimbursement rates on any of these codes, use the CMS Physician Fee Schedule lookup tool on the CMS website. Rates update annually, and the tool allows filtering by geographic area and facility versus non-facility setting.
Staying Current as Policy Changes
CMS updates the Medicare Physician Fee Schedule through annual rulemaking. Proposed rules typically publish in summer, with final rules released in fall and taking effect January 1. Social workers with any stake in reimbursement policy should monitor the CMS rulemaking website for Physician Fee Schedule updates each cycle.
The National Association of Social Workers tracks final rules, advocacy wins, and billing guidance specific to the profession. NASW and its state chapters also publish LCSW-specific billing guides that translate CMS policy into practical guidance. These are worth bookmarking alongside the primary CMS sources, not as a replacement for them. Additionally, meeting continuing education requirements in your state helps ensure you stay current on evolving billing regulations and clinical standards.
Reimbursement rules are not static, and gaps between what social workers do and what they can bill for remain an active policy issue. Staying informed on both the current rules and the direction of advocacy efforts is practical professional knowledge, not just regulatory housekeeping.
Related Articles
Case Studies: Social Work Cost Savings by Healthcare Setting
Real-world programs demonstrate measurable cost savings when social workers are embedded across healthcare settings. The following case studies illustrate the financial impact by facility type.
Acute-Care Hospitals: Care Transitions Programs
The CMS Community-Based Care Transitions Program placed social workers and care transition coaches in acute-care hospitals to conduct structured needs assessments, discharge planning, medication reviews, and patient and family education. By arranging community services for high-risk Medicare patients moving from hospital to home, the program cut all-cause 30-day readmissions by 8% and generated Medicare savings of roughly $300 per beneficiary per quarter.1
A similar initiative, the Evansville/Vanderburgh County Care Transitions Collaborative, used social workers and nurses as transition coaches for high-risk Medicare patients. Through in-hospital assessments, home visits, medication reconciliation, social determinant screening, and linkage to community resources, the collaborative reduced 30-day readmissions by 15% and produced estimated net savings of $2.1 million to Medicare.2
Primary Care Clinics: IMPACT Collaborative Care
The IMPACT model embeds depression care managers, often social workers, in primary care settings to deliver systematic screening, psychotherapy, and coordinated behavioral health support. Over four years, the multi-site randomized trial found $3,363 lower total healthcare costs per patient, returning about $6.50 for every $1 invested.3
Federally Qualified Health Centers (FQHCs)
FQHCs that integrated MSW-trained behavioral health care managers saw significant reductions in depression symptoms alongside lower total medical costs of $500 to $1,000 per patient per year. These healthcare social workers track outcomes, deliver brief psychotherapies, and connect patients to community resources.3
Tertiary Hospitals: Palliative Care Consultation Teams
Interdisciplinary palliative care teams that include a social worker in hospice and acute-care roles conduct goals-of-care conversations, psychosocial assessments, family meetings, and discharge planning to home hospice. Multi-site cost analyses show hospital cost reductions of 14 to 22% per admission, translating to $1,696 to $4,908 in savings per admission.3
Health Plans and ACOs: Complex Care Management
In Medicare Advantage and Medicaid plans, social workers serving as care managers for high-risk enrollees deliver intensive outreach, home visits, psychosocial assessments, and coordination with primary care providers and specialists. These programs achieve 10 to 20% reductions in inpatient admissions, 15 to 25% drops in ED visits, and total cost reductions of roughly 7 to 12% for targeted cohorts.3
Social workers do more than improve patient satisfaction: they directly protect a health system's bottom line. By preventing the costliest events in healthcare, including unplanned readmissions, avoidable emergency visits, and extended inpatient stays caused by unresolved social barriers, they turn upstream intervention into measurable savings.
Healthcare Social Worker Salary and Job Outlook
Healthcare social workers (SOC 21-1022) earn a solid income relative to the broader social work field, and demand is growing faster than the average for all occupations. The figures below reflect national data from the Bureau of Labor Statistics, May 2023 Occupational Employment and Wage Statistics release, along with employment projections. For state-level pay comparisons, see the salary-by-state table that follows.
| Occupation | National Median Salary | 25th Percentile | 75th Percentile | Total Employment (May 2023) | Projected Growth Rate |
|---|---|---|---|---|---|
| Healthcare Social Workers | $68,090 | $55,360 | $83,410 | 185,940 | 9.6% (2022 to 2032) |
| Child, Family, and School Social Workers | $58,570 | $47,480 | $74,060 | 382,960 | N/A |
| Mental Health and Substance Abuse Social Workers | $60,060 | $46,550 | $78,980 | 125,910 | N/A |
| All Social Workers | $61,330 | $48,680 | $78,500 | 759,740 | 6% (2024 to 2034) |
Healthcare Social Worker Salary by State
Compensation for healthcare social workers varies significantly by state, driven by cost of living, demand, and local reimbursement structures. The table below shows median annual wages for healthcare social workers (BLS occupation code 21-1022) across the 15 highest-paying states and territories in the dataset. All figures are state-specific medians, not national averages.
| State | Total Employment | Median Annual Wage | 25th Percentile Wage | 75th Percentile Wage |
|---|---|---|---|---|
| California | 19,680 | $92,970 | $67,880 | $122,200 |
| District of Columbia | 490 | $92,600 | $77,790 | $105,750 |
| Oregon | 2,050 | $85,150 | $66,650 | $102,390 |
| Hawaii | 680 | $84,640 | $58,270 | $95,520 |
| Connecticut | 2,010 | $81,900 | $73,200 | $97,140 |
| New Jersey | 4,390 | $81,710 | $66,100 | $100,200 |
| Rhode Island | 570 | $79,460 | $63,450 | $91,510 |
| Vermont | 300 | $78,390 | $65,340 | $92,780 |
| New Hampshire | 530 | $78,000 | $69,710 | $89,790 |
| Alaska | 290 | $77,990 | $60,200 | $88,440 |
| Nevada | 1,070 | $76,280 | $61,150 | $89,990 |
| Washington | 4,970 | $75,670 | $58,330 | $95,170 |
| Maine | 590 | $72,520 | $63,750 | $77,780 |
| Utah | 1,930 | $72,370 | $57,930 | $89,690 |
| Minnesota | 2,530 | $72,330 | $60,830 | $84,490 |
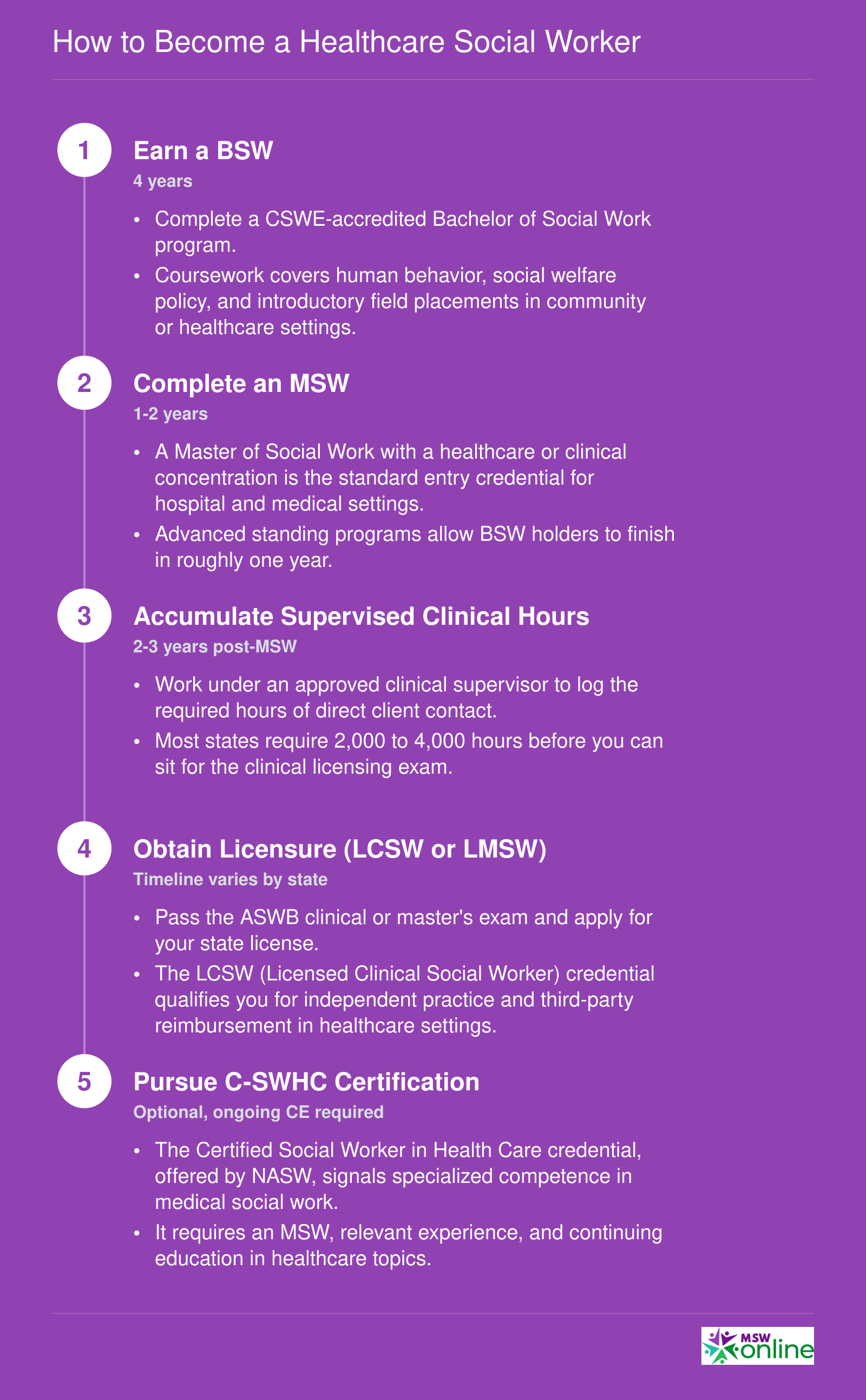
How to Become a Healthcare Social Worker
Healthcare social work requires a clear credentialing ladder. Each step builds clinical knowledge and professional authority, positioning you to work in hospitals, integrated care teams, and community health organizations.
The Future of Social Work in Healthcare: Value-Based Care, ACOs, and Telehealth
Healthcare payment in the United States is shifting away from a model that rewards volume toward one that rewards outcomes. That single change is reshaping the financial logic of hiring social workers.
Value-Based Care Makes Social Work a Revenue Strategy
Under fee-for-service, a hospital got paid whether a patient returned to the emergency room three times or zero. Under value-based contracts, bundled payments, and Medicare Advantage quality bonuses, avoidable readmissions and unmanaged social risk directly reduce revenue. Preventing those events is now a financial priority, not just a clinical aspiration. That gives health systems a concrete business reason to embed social workers into care teams.
The CMS Innovation Center has set a goal of moving all Medicare beneficiaries into accountable care relationships by 2030.1 Its core strategy leans on care management, behavioral health integration, and interventions targeting health-related social needs. Social work in mental health sits at the intersection of all three.
ACO REACH, CMS's advanced accountable care model, has required participating organizations to maintain health equity plans and to make targeted engagement efforts toward vulnerable populations.2 A 2026 financial methodology update reinforces this direction.2 According to NAACOS, a majority of ACOs now employ social workers, frequently placing them in primary care teams and population health departments to manage high-risk patient panels and close care gaps.1
The newer ACCESS model goes further, tying payment explicitly to clinical and equity-related outcomes. It covers health-related social needs screening, navigation, and related services, and it measures performance partly on whether identified social needs are actually resolved.3
Telehealth Social Work: Pandemic Flexibility Becomes Permanent Policy
The pandemic forced a rapid expansion of telehealth, and much of it stuck. Medicare permanently extended audio-only behavioral health coverage and made permanent the ability to bill for mental health services at federally qualified health centers and rural health clinics via telehealth.1 The home is now a recognized originating site for behavioral health telehealth under Medicare. Social work services are covered under Medicare telehealth billing.1
In practice, this means remote psychosocial assessments, virtual discharge follow-up calls, and tele-behavioral health sessions are no longer workarounds. They are standard, reimbursable care. Professionals interested in delivering these services remotely may also consider building a private practice social work model.
SDOH Screening Requirements Create Structured Demand
CMS has actively promoted the use of ICD-10 Z-codes to document social determinants of health, pushing for their routine use across care settings from 2023 onward.1 A CMS quality measure now tracks the percentage of patients screened for housing instability, food insecurity, transportation barriers, utility needs, and interpersonal safety.1 Documenting and acting on those screens requires staff with training in community resources, benefit navigation, and psychosocial intervention. That is, in short, a job description for a medical social worker.
Taken together, these policy shifts do not just make room for social workers in healthcare. They create structured, reimbursable, and increasingly measured demand for what social workers do.
Frequently Asked Questions About Social Work and Healthcare Costs
Below are answers to some of the most common questions about how social workers contribute to healthcare delivery, lower costs, and improve patient outcomes. Each answer draws on evidence and data points discussed throughout this article.
Explore More
- Bilingual Social Worker
- Continuing Education for Social Workers
- COVID-19 Guide for Social Workers
- CSWE Accreditation
- DSW vs. PhD in Social Work
- Environmental Social Work
- Free Implicit Bias Tests & Training Resources
- How Long Does It Take to Become a Social Worker?
- How to Find a Social Work Job
- Levels of Social Work Licensure
- LGBTQIAP in Social Work
- Mental Health & Homelessness
- Micro, Mezzo & Macro Social Work
- MSW Admission Requirements
- MSW Scholarships
- MSW Specializations
- MSW vs. MSSW
- Remote Resources for Mental Health Workers
- Social Work & Food Insecurity
- Social Work & Gun Violence Prevention
- Social Work Ethics
- Social Work Field Placement Guide
- Social Work Grants
- Social Work Internships
- Social Work Theories & Practice Models
- Social Work Volunteer Opportunities
- Social Work vs. Counseling
- Social Work vs. Psychology
- Social Work vs. Sociology
- Social Worker Salary Guide
- Social Worker vs. Therapist
- Social Worker's Guide to Cyberbullying
- Student Mental Health & Social Work on College Campuses
- What Can You Do With an MSW Degree? Careers & Salaries
- Why Is Research Important in Social Work? A Complete Guide
- Women in Social Work Leadership