Points of interest…
- Chronic loneliness raises an older adult's risk of dementia by roughly 50 percent and increases premature mortality comparably to smoking.
- Cognitive behavioral therapy and structured social skills training show the strongest evidence for reducing loneliness scores in seniors.
- Geriatric social workers use validated screening tools to distinguish temporary loneliness from clinical isolation requiring intervention.
- Caregivers should identify the specific barrier, whether mobility, cognition, or geography, before choosing any intervention strategy.
Roughly one in four Americans aged 65 and older reports feeling lonely on a regular basis, and the health toll is not abstract: chronic loneliness raises the risk of dementia by 50 percent and the risk of premature death by 26 percent, rivaling the harm of smoking 15 cigarettes a day. These are not inevitable outcomes of aging.
Evidence-based interventions, from cognitive behavioral therapy adapted for isolation to structured social prescribing programs, measurably reduce loneliness scores in controlled trials. Families, social workers, and older adults themselves each have concrete levers to pull. The challenge is matching the right intervention to the right barrier, whether that barrier is limited mobility, cognitive decline, rural geography, or simple lack of awareness that help exists. The sections below break down the crisis by the numbers, rank interventions by strength of evidence, and offer practical steps organized by situation, so that social work research and real-world action connect at every level.
Why Loneliness Is a Growing Crisis for Older Adults
Feeling lonely and being isolated are not the same thing, yet both are accelerating among older Americans, and each demands a distinct response. Loneliness is the subjective gap between the social connection a person wants and what they actually have. Social isolation is the measurable absence of contact: few relationships, infrequent interaction, limited community participation. A person can feel deeply lonely in a crowded assisted-living facility, just as someone living alone in a rural county may feel perfectly content. Understanding this distinction matters because the interventions differ. Loneliness often responds to quality-of-connection strategies, while isolation typically requires structural changes such as transportation, housing, or digital access.
How Many Older Adults Are Affected
The numbers are stark. A 2024 survey from the University of Michigan found that roughly one in three adults ages 50 to 80 reported chronic loneliness, and 29 percent met criteria for social isolation.1 AARP's 2024 loneliness epidemic survey, which captured adults 45 and older, placed the loneliness rate at 40 percent overall, with men (42 percent) reporting higher rates than women (37 percent).2 Income amplifies the problem: 63 percent of adults 45 and older earning under $25,000 a year described themselves as lonely. Among those reporting fair or poor physical health, the rate hit 59 percent, and those with a mental health condition reached 58 percent.2 Approximately 24 million Americans over 50 now live alone, a figure that climbs to roughly half of all adults 75 and older.3
The Health Toll, by the Numbers
The U.S. Surgeon General's 2023 advisory on the loneliness epidemic framed social disconnection as a public health threat on par with smoking 15 cigarettes a day. The data behind that comparison is sobering:4
- Premature death: Socially disconnected older adults face a 25 to 30 percent higher risk of mortality.
- Dementia: Social isolation raises dementia risk by an estimated 40 to 50 percent.
- Heart disease: Isolated older adults show a 29 percent increase in coronary heart disease risk.
- Stroke: The same population faces a 32 percent elevated stroke risk.
These are not small effect sizes. They rival or exceed the risks associated with obesity, physical inactivity, and air pollution.
Structural Forces Driving the Crisis
Several converging trends explain why the problem keeps growing rather than stabilizing:
- Retirement: Leaving the workforce eliminates daily social structures that many people relied on for decades without building replacements.
- Spousal loss: Widowhood is one of the strongest predictors of isolation, and women, who on average live longer, are disproportionately affected. About 33 percent of women over 50 live alone compared with 20 percent of men.3
- Mobility decline: Chronic pain, falls, and loss of driving ability shrink a person's social radius to whatever is within walking distance or available through others.
- Geographic dispersion of families: Adult children increasingly live hours or states away, reducing the frequency of in-person contact that phone calls and video chats only partly replace.
- Rural depopulation: Shrinking rural communities lose the gathering places, senior centers, faith communities, and healthcare access that once kept older residents connected.
None of these drivers is reversible at the individual level, which is exactly why loneliness in older adults is now treated as a systemic crisis rather than a personal failing. Professionals such as geriatric social workers are increasingly central to coordinating responses. The sections that follow lay out what the evidence says actually works, and what caregivers, social workers, and older adults themselves can do about it.
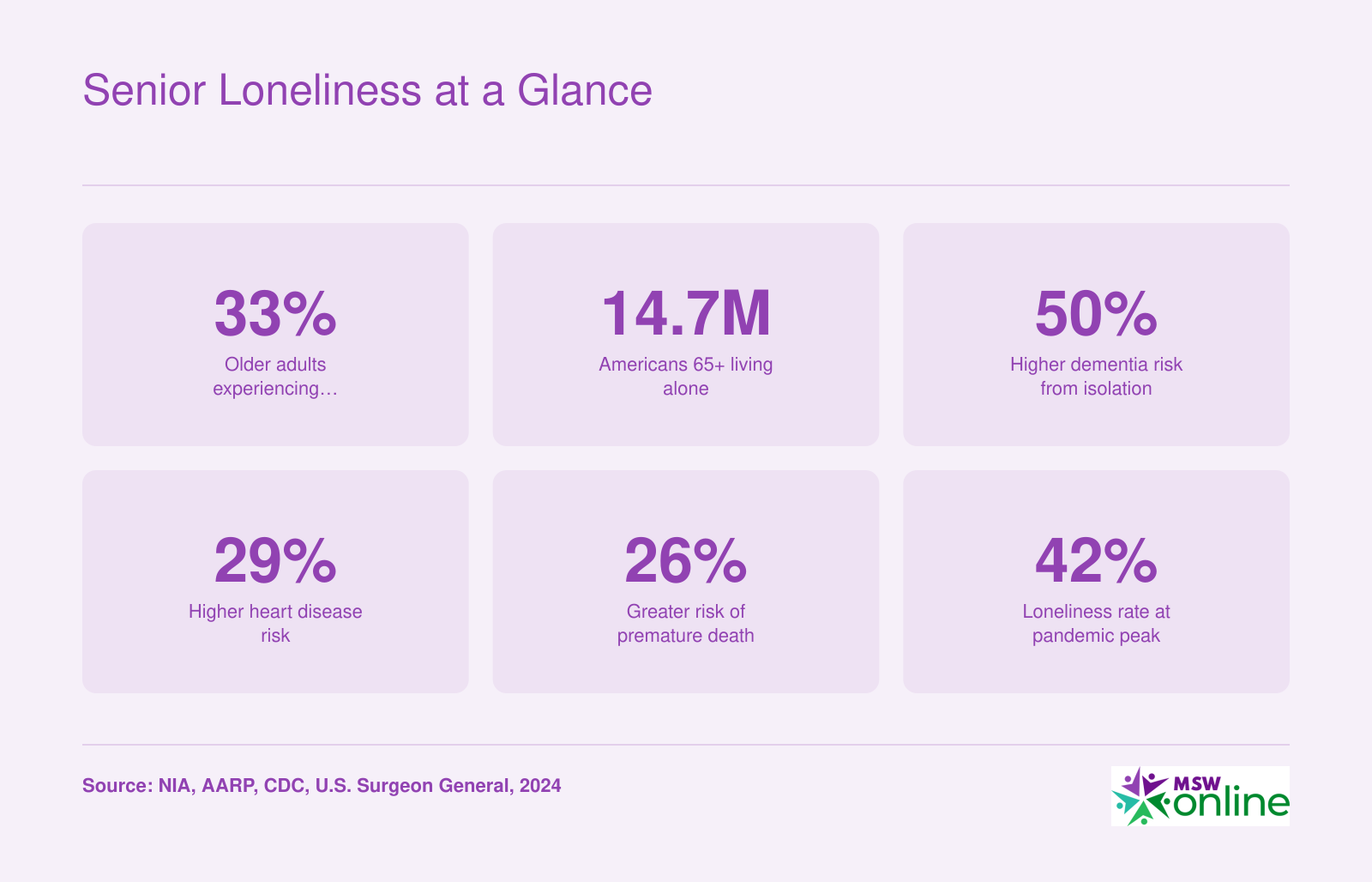
Senior Loneliness at a Glance
Loneliness among older Americans is not just an emotional burden. It is a measurable public health crisis with direct links to chronic disease, cognitive decline, and premature death. The figures below capture the scope of the problem.
Recognizing the Signs: Normal Loneliness Vs. Clinical Concern
A growing body of research now distinguishes transient loneliness from chronic social isolation as separate health risks, reshaping how practitioners screen for severity. In social work, early differentiation between normal adjustment-related loneliness and pathological withdrawal is critical because untreated social disconnection can accelerate cognitive decline, weaken immune function, and raise mortality risk to levels comparable to smoking 15 cigarettes a day. Recognizing where someone falls on this spectrum empowers families and caregivers to intervene appropriately.
Situational Loneliness: What's Normal
Loneliness does not always signal a disorder. After a major life transition, such as moving to a retirement community, retiring from a lifelong career, or losing a spouse, older adults may experience transient feelings of emptiness and solitude. These feelings often ease within a few weeks as the person builds new routines and reconnects socially. During this phase, the individual typically still engages with familiar activities, maintains personal hygiene, and can articulate a desire to feel more connected. Brief periods of sadness or nostalgia are common and do not warrant clinical alarm. Normalizing this experience can reduce anxiety for both the older adult and their families, reinforcing that loneliness is a human emotion, not a permanent condition.
When Loneliness Becomes a Clinical Concern
Red flags emerge when loneliness shifts from situational discomfort to persistent, life-disrupting withdrawal. Clinicians trained in geriatric social work look for patterns that endure longer than two to three weeks and interfere with daily functioning. Key warning signs include:
- Persistent withdrawal: Refusing social contact or losing interest in previously enjoyed activities for more than several weeks.
- Appetite and sleep changes: Significant weight loss or gain, insomnia, or excessive sleeping that deviates from the person's baseline.
- Neglect of hygiene: Skipping bathing, wearing soiled clothes, or letting the home become disorganized to the point of safety concerns.
- Expressions of hopelessness: Repeated statements like "I'm a burden," "There's no point," or "I'd rather not wake up."
- Increased alcohol or medication misuse: Using substances to fill time or numb feelings of isolation.
- Cognitive decline: Noticeable memory lapses, confusion, or trouble concentrating that seem to worsen alongside social isolation.
These signs often overlap; many older adults exhibit several simultaneously. The presence of even one, if intense and enduring, warrants attention, but a cluster of three or more strongly suggests that professional support is needed.
A Simple Screening Framework
Families can use a straightforward rule: if the older adult shows three or more of the red flags above or makes any mention of self-harm, a clinical referral is overdue. Appropriate first steps include contacting the primary care provider, a geriatric psychiatrist, or a licensed clinical social worker who can conduct a thorough psychosocial assessment. Two validated screening tools can help structure these conversations:
- The UCLA Loneliness Scale (short form) asks three simple questions about felt companionship, exclusion, and isolation. It is widely used in both research and primary care settings to quantify loneliness severity.
- The De Jong Gierveld scale captures both emotional and social loneliness dimensions, making it especially useful for pinpointing whether the individual lacks intimate connections or broader social integration.
These instruments do not replace clinical judgment but offer a concrete way to measure what can feel abstract. When scores are elevated, or when the older adult cannot respond to the questions meaningfully, a licensed social worker can coordinate a safety plan, connect the individual to evidence-based loneliness interventions, and address underlying medical or psychiatric contributors. Catching loneliness at this threshold can prevent a cascade of worsening health and restore a sense of purpose.
Questions to Ask Yourself
Most Effective Loneliness Interventions for Seniors, Ranked by Evidence
Not all loneliness interventions work equally well. Systematic reviews and meta-analyses published over the past five years let us rank approaches by their measured effect on loneliness scores (typically the UCLA Loneliness Scale or de Jong Gierveld scale). The picture that emerges from a 2024 Frontiers in Public Health review, Cochrane reviews, and related syntheses is clear: psychological and relational interventions consistently outperform information-only programs.
How the Evidence Ranks Interventions
The strongest support, in descending order of typical effect size reported across recent meta-analyses, falls roughly like this:
- Cognitive behavioral therapy (CBT) and psychological therapies: Adapted CBT targeting maladaptive social cognitions (the belief that others do not want to engage) tends to produce the largest and most durable reductions in loneliness scores. Reminiscence therapy and acceptance-based approaches also show moderate effects.
- Animal-assisted therapy: Structured visits with trained therapy animals show moderate to large short-term effects on loneliness and depressive symptoms, particularly in long-term care settings. Effects on community-dwelling seniors are smaller but still positive.
- Group-based social support and skill-building activities: Programs that combine social contact with a shared purpose (exercise groups, art classes, cognitive training) outperform groups organized purely around socializing. The shared task gives quieter participants something to do besides perform.
- Befriending and one-to-one volunteer visiting: Effects are modest but reliable, especially for homebound seniors. Telephone befriending has weaker evidence than in-person visits but still beats no contact.
- Education-only programs and information mailings: Lowest effect sizes. Knowing about loneliness does not fix it.
Where to Verify Current Rankings
These rankings shift as new trials publish. Three sources worth checking directly:
- The Cochrane Library and Frontiers in Public Health for full systematic reviews with effect sizes and GRADE evidence ratings.
- The National Institute on Aging (nia.nih.gov) and Administration for Community Living (acl.gov) for evidence-based program directories and funding signals indicating which interventions agencies are scaling.
- The American Psychological Association and Gerontological Society of America for practice guidelines that translate the research into clinical recommendations.
For a custom search, PubMed and Google Scholar both respond well to queries like "loneliness interventions older adults meta-analysis effect size," filtered to systematic reviews from 2020 through 2025.
What This Means in Practice
If you can only invest in one approach, prioritize a structured group activity with a defined task, ideally led by someone trained to draw out quieter members. If clinical depression or social anxiety is in the mix, add a referral for CBT with a therapist experienced in geriatric care. A mental health social worker can be especially effective in coordinating these referrals and ensuring continuity of care. Save passive interventions (newsletters, drop-in centers without programming) for supplementary roles, not the centerpiece.
Related Articles
Practical Solutions by Situation: Mobility-Limited, Cognitive Impairment, and Rural Seniors
Not every older adult faces loneliness for the same reasons, so effective interventions must be tailored to the specific barriers a person encounters. Below are targeted strategies organized by three common situations.
Mobility-Limited Seniors
Physical limitations should not translate into social disappearance. Consider these approaches:
- Schedule regular video calls with family and friends using tablets with simplified interfaces.
- Arrange in-home visits through volunteer companion programs or faith-based outreach teams.
- Explore adaptive transportation services, such as wheelchair-accessible shuttles, offered by local Area Agencies on Aging.
- Introduce doorstep or porch-based social gatherings with neighbors when weather permits.
For homebound seniors nearing end of life, a hospice social worker can coordinate emotional support and help families maintain meaningful connection during a difficult transition.
Seniors with Cognitive Impairment
Dementia and other cognitive conditions create unique barriers to social engagement, but structured interaction remains beneficial.
- Use reminiscence-based activities, such as photo albums and familiar music, to spark conversation.
- Connect caregivers with memory care day programs that offer supervised group interaction.
- Encourage simple, repetitive social rituals (a daily greeting, a shared meal) that build comfort without overwhelming cognitive resources.
- Train family members and volunteers in validation communication techniques that prioritize emotional connection over factual accuracy.
Professionals interested in supporting this population can pursue social work certifications that deepen expertise in aging and cognitive health.
Rural Seniors
Geographic isolation amplifies loneliness when the nearest neighbor, grocery store, or community center is miles away.
- Leverage telehealth and online counseling platforms to provide consistent social and mental health support.
- Organize telephone "buddy systems" through local churches, granges, or cooperative extension offices.
- Advocate for mobile library and wellness programs that bring activities directly to remote areas.
- Partner with rural mail carriers or utility workers for wellness check-in programs.
In every situation, the goal is the same: reduce the gap between a senior's desire for connection and their ability to access it. Matching the intervention to the barrier, whether physical, cognitive, or geographic, dramatically improves the odds of success.
Effective support starts by identifying the primary barrier your loved one faces: limited mobility, cognitive changes, geographic isolation, or personality. A social group does nothing for someone who cannot get there. Pinpoint the obstacle first, then choose an intervention that directly addresses it, and you will avoid wasted effort.
What Caregivers and Family Members Can Do
Watching a parent or grandparent withdraw from the world is distressing, and the impulse to help can quickly collide with the reality of distance, time, and money. A structured approach cuts through that paralysis.
Step 1: Identify the Barrier
Before choosing any intervention, name the obstacle that is actually driving isolation. Four categories cover most situations:
- Physical: Mobility limits, chronic pain, or transportation gaps that prevent the senior from leaving home
- Emotional: Grief, depression, anxiety, or a general reluctance to engage after a major life change
- Geographic: The senior lives in a rural area or far from family, so in-person contact is infrequent
- Cognitive: Early dementia or mild cognitive impairment that makes novel social settings confusing or overwhelming
The barrier determines the solution. Enrolling a mobility-limited senior in a telephone befriending program is more practical than urging them to attend a weekly class. Pushing a grieving widow into group activities before she has processed her loss may backfire; a one-on-one counseling referral fits better. In many cases, a family counseling approach helps relatives coordinate a unified care plan.
Step 2: Match the Intervention to the Barrier
Once you have identified the barrier, look at evidence-based options from least to most intensive. For families acting immediately, several low-cost moves require almost no lead time:
- Schedule video or phone calls at a fixed time each week. Predictability matters as much as frequency; a Tuesday-at-3 call the senior can count on reduces the unpredictability that feeds anxiety.
- Ask a grandchild or younger relative to spend one afternoon teaching the senior to use a tablet or smartphone. Familiarity with the device removes the intimidation that keeps many older adults off video platforms entirely.
- Contact the nearest senior center and request a free trial day. Most centers welcome first visits at no charge, and a familiar face on the first visit (a neighbor, a volunteer escort) improves the chance the senior returns.
- Organize a simple meal rotation with two or three neighbors. Meals involve brief, natural conversation without the pressure of a formal social event, and they provide a reliable check-in for the household.
Step 3: Weigh Cost and Access
Cost is a real filter. Senior center programs, Area Agencies on Aging services, and telephone reassurance lines are generally free or sliding-scale. The Eldercare Locator (a federally funded service reached at 1-800-677-1116) connects families to local resources by ZIP code and is particularly useful for long-distance caregivers who need a local proxy to check in regularly. Area Agencies on Aging can arrange care coordination, transportation, and socialization programs that a distant family member cannot easily manage alone.
For seniors whose isolation has tipped into clinical depression or anxiety, Medicare Part B covers individual psychotherapy, group psychotherapy, psychiatric evaluations, medication management, family counseling, and intensive outpatient programs.1 After the 2026 Part B deductible of $283 is met, the coinsurance rate for outpatient mental health services is 20 percent, meaning Medicare covers the remaining 80 percent when the provider accepts assignment.2 Annual depression screenings are covered at no cost to the beneficiary.1 Note that the temporary expansion of telehealth mental health coverage under Part B ended January 30, 2026; caregivers should confirm current telehealth availability directly with Medicare or the provider.2
For seniors who qualify for both Medicare and Medicaid (dual-eligible), PACE (Program of All-inclusive Care for the Elderly) can cover social day care along with medical services. PACE programs vary by location, so checking availability through the local Area Agency on Aging is the practical first step.
When You Live Far Away
Long-distance caregiving carries a particular weight of guilt, but the logistics are manageable with the right intermediaries. Three resources worth bookmarking:
- Eldercare Locator: A free federal service that identifies local agencies and programs by ZIP code
- Area Agencies on Aging: Local offices funded under the Older Americans Act that coordinate meals, transportation, and socialization programs at little or no cost
- AARP Caregiver Resource Center: Offers guides on navigating Medicare mental health coverage and connecting with community services
None of these replace consistent personal contact, but they extend a family's reach considerably when geography makes in-person visits infrequent.
How Social Workers Address Senior Loneliness
Social workers are front-line professionals who transform senior loneliness from an invisible crisis into a solvable problem through systematic assessment, resource navigation, and compassionate intervention. Trained in a person-in-environment framework, geriatric social workers evaluate not only the individual's emotional state but also the web of relationships, housing, mobility, and community supports that sustain connection. They conduct comprehensive psychosocial assessments to pinpoint the root causes of isolation, whether arising from recent widowhood, chronic illness, transportation barriers, or untreated hearing loss, and then build individualized plans that connect older adults to resources like senior centers, friendly visitor programs, meal delivery services, and accessible transportation.
Social workers are also skilled facilitators of evidence-based interventions. They often run or refer clients to support groups tailored for bereaved spouses, caregivers, or those with chronic conditions, creating safe spaces where shared experience reduces stigma and fosters belonging. When loneliness feeds into maladaptive thought patterns, like "no one cares" or "I'm a burden," they may deliver cognitive behavioral therapy (CBT) directly or coordinate with licensed therapists, helping seniors reframe negative beliefs and rebuild social confidence. For homebound individuals, social workers advocate persistently: coordinating telehealth options, in-home volunteer visitors, or pet therapy services to pierce the walls of isolation.
Practice Settings Where Senior Loneliness is Tackled
In hospitals, social workers are central to discharge planning, assessing whether a patient returning home alone has adequate support and connecting them with follow-up services to prevent readmission and post-discharge loneliness. Nursing homes and assisted living facilities employ social workers to foster community within the residence, organizing activities, mediating family involvement, and ensuring residents do not retreat into solitary routines. Area Agencies on Aging place social workers at the hub of community-based services, linking isolated seniors to local transportation, nutrition programs, and volunteer companions. Community mental health centers and hospice organizations rely on social workers to address the emotional and practical dimensions of end-of-life isolation, working with families and patients to maintain dignity and connection during terminal illness.
Loneliness vs. Depression: A Critical Distinction
A critical skill social workers bring to loneliness interventions is the ability to differentiate between normal loneliness and clinical depression. While loneliness is a subjective distressing perception of disconnection, depression is a mood disorder with neurobiological underpinnings that may include anhedonia, sleep disturbance, and hopelessness. The screening approaches described previously in this article equip caregivers and families with initial signals, but social workers apply validated tools like the Geriatric Depression Scale and clinical interviews to make nuanced distinctions. When depression is present, they refer to psychiatric social workers or primary care providers for medication evaluation while continuing to address the social and environmental contributors to loneliness.
Geriatric Social Work as a Career Path
For students and professionals considering this field, the geriatric social work specialization offers a direct pathway into meaningful work. MSW programs with aging concentrations and post-graduate certificates in gerontology prepare social workers to navigate Medicare, Medicaid, and the aging services network. As the population over 65 grows, demand for clinically trained social workers who can combat senior loneliness will expand across healthcare and community settings, making it a career in social work with both deep personal impact and professional resilience.
Technology and Digital Solutions for Staying Connected
The conversation around tech and senior loneliness has shifted in the past two years: researchers no longer ask whether devices help, but which formats help, for whom, and in what combination with human contact. A 2026 meta-analysis of technology-based loneliness interventions found a modest pooled effect (SMD around -0.21)1, while digital health interventions overall landed closer to -0.39, and cognitively focused digital programs reached -0.82.2 The takeaway: technology works, but the design matters more than the device.
Main Categories of Tools
- Simplified video-calling devices: GrandPad and Meta Portal strip away the friction of standard tablets, offering one-touch calls, large icons, and family-managed contact lists. ElliQ, a tabletop companion robot, reports quality-of-life improvements in roughly 90% of users in company-published data (independent replication is still limited).3
- Senior-friendly social apps: Stitch, Senior Planet Community, and curated Facebook groups create peer networks without the overwhelm of mainstream platforms.
- Virtual senior centers: Programs like Well Connected (Covia) and Senior Planet Online offer live group classes, discussion circles, and exercise sessions by phone or video. Evidence suggests interpersonal interaction via technology produces stronger effects (around -0.60 Hedges' g) than passive content consumption.4
- Telehealth counseling: Medicare now covers video-based mental health visits, opening grief and depression treatment to homebound seniors.
Closing the Digital Literacy Gap
Roughly a quarter of adults over 65 still report low confidence with internet-connected devices. Older Adults Technology Services (OATS), now operating under AARP as Senior Planet, runs free training nationwide. UC Berkeley's Senior Vitality Program demonstrated that structured digital literacy training can raise technology confidence by 60% while simultaneously reducing loneliness by 60%.5 Public libraries increasingly host one-on-one tech coaching, and several states (California, New York, Massachusetts among them) fund tablet lending or distribution for low-income seniors. The Affordable Connectivity Program's wind-down in 2024 left gaps that Lifeline and local nonprofits are still scrambling to fill.
For professionals interested in delivering telehealth services to older adults, understanding the foundations of online counseling is an important first step.
What the Evidence Actually Says
Video calls reduce loneliness, but the effect shrinks for the most severely isolated, where in-person contact remains superior. Hybrid models, where technology bridges between visits rather than replacing them, perform best. Interventions that involve family members directly show the strongest results (-0.69 Hedges' g).4
Practical Cost Guidance
Free options (WhatsApp, Zoom, FaceTime) work well when a family member handles setup. Refurbished tablets run $50 to $100. Qualifying low-income seniors can receive free devices through GetSetUp partnerships, state aging departments, and some Medicare Advantage plans that now bundle tablets with care coordination.
Programs, Organizations, and Resources for Isolated Seniors
A national safety net of programs exists specifically to reach isolated older adults, ranging from phone hotlines and home-delivered meals to volunteer-staffed friendly visitor services and comprehensive medical-social programs. Knowing which door to knock on, and what each costs, makes the difference between a parent staying home alone and getting connected within a week.
National Programs Worth Knowing
- AARP Foundation Connect2Affect: A free online platform from the AARP Foundation offering a self-assessment to gauge isolation risk, educational content, and a directory pointing users to local assistance. No age or income requirement. Access through the Connect2Affect website or AARP's help line. Active and updated through 2026.1
- Eldercare Locator: A free public service of the U.S. Administration on Aging that connects callers to local aging services. Call 1-800-677-1116 (weekdays) or use the website. No eligibility restrictions. This is the single best starting point for families who don't know where to begin.
- Area Agencies on Aging (AAAs): A nationwide network of roughly 600 regional agencies that coordinate transportation, meals, caregiver respite, senior center programming, and case management. Most core services are free or sliding-scale based on income. Find your local AAA through the Eldercare Locator.
- PACE (Program of All-Inclusive Care for the Elderly): A Medicare/Medicaid program for adults 55+ who meet their state's nursing home level-of-care standard but can live safely in the community. PACE bundles medical care, adult day health, transportation, and social engagement. Cost depends on payer source: free for dual-eligibles, premium-based for Medicare-only enrollees. Search the National PACE Association directory by ZIP code.
- Meals on Wheels: Beyond food, the daily visit functions as a wellness check and human contact, often the only face-to-face interaction a homebound senior has. Many local programs also run telephone reassurance and friendly visitor add-ons. Eligibility and cost vary by chapter; many use sliding-scale donations. Find a provider through mealsonwheelsamerica.org.
- AmeriCorps Seniors (formerly Senior Corps): Engages adults 55+ as volunteers through the RSVP, Foster Grandparent, and Senior Companion programs. Volunteering itself is a proven loneliness intervention, and the Senior Companion program also pairs volunteers with isolated peers. Free to participate; some roles include a small stipend for lower-income volunteers.
Finding Local Help Fast
Two phone numbers solve most search problems. Dial 211 for a trained operator who can route callers to local food, transportation, mental health, and senior services in any U.S. community. Dial 1-800-677-1116 (Eldercare Locator) for aging-specific referrals. Both are free, confidential, and available in multiple languages. For families navigating cost questions, the general rule is this: federally funded programs (AAA services, Eldercare Locator, AmeriCorps) are typically free or sliding-scale, PACE is insurance-covered through Medicare and Medicaid, and Meals on Wheels operates on suggested donations with no one turned away for inability to pay.
Frequently Asked Questions About Senior Loneliness
Below are answers to the questions caregivers, family members, and older adults ask most often about senior loneliness. Each answer points back to relevant sections of this guide for deeper detail.