Points of interest…
- Medicare telehealth mental health visits jumped from 2.1 percent before the pandemic to 42.9 percent by 2024.
- Message-based therapy matched video therapy on depression outcomes in an 850-adult randomized controlled trial.
- HIPAA requires end-to-end encryption and a signed Business Associate Agreement for every telehealth platform.
- Only four states were issuing Counseling Compact privileges as of April 2026, limiting multistate practice.
What exactly separates online counseling from the growing number of mood-tracking apps and AI chatbots marketed as mental health tools? The distinction matters. Online counseling refers to licensed mental health services delivered by credentialed professionals through video, phone, or asynchronous messaging platforms that meet clinical and legal standards. Unlike unregulated wellness apps, these sessions involve diagnosis, treatment planning, and documentation governed by state licensing boards and federal privacy law.
In-person therapy still accounts for the majority of clinical encounters, but telehealth's share of mental health visits has surged from roughly 2 percent before the pandemic to over 40 percent in recent years. For social workers, that shift has created both new practice models and new compliance demands around HIPAA, interstate licensure compacts, and platform selection. Those considering a career in social work will find telehealth competency increasingly central to the profession.
How Does Online Counseling Work?
Online counseling shifts the therapeutic frame from a shared room to a screen, yet the core process remains intentionally familiar. The journey begins with digital intake forms, privacy consents, and a brief tech-check before you meet a therapist. This upfront structure trades physical proximity for logistical clarity, and most platforms guide you through each step.
The Client Journey: From Sign-Up to Session
- Intake and matching: After completing a questionnaire about symptoms, history, and preferences, the platform matches you with a licensed therapist, usually within one to three days. You can often request a new match if the fit feels off.
- Platform onboarding and scheduling: You create an account on a HIPAA-compliant portal, verify your identity, and pick a session time. Built-in calendars handle time zones automatically.
- The session itself: At the appointed time, you log in to a virtual waiting room. The therapist opens the session, and you talk via video, phone, or text. Sessions typically last 45 to 55 minutes. Afterward, you may receive a summary or homework assignments through the platform.
Video, Phone, and Text: Choosing a Modality
- Synchronous video is the closest to traditional office visits and is best for deeper emotional processing, couples work, or when reading nonverbal cues matters.
- Phone sessions work well when visual privacy is limited or internet is unstable, and some clients find the audio-only format less intimidating.
- Asynchronous text or messaging lets you send messages anytime, and your therapist replies within a set window. This modality suits ongoing support between live sessions or clients who process slowly, but it lacks immediacy for acute distress.
Devices, Internet, and Space: What You Need
- Hardware: A computer, tablet, or smartphone with a working camera and microphone. For video, a screen large enough to see facial expressions is ideal.
- Internet: A stable broadband connection with at least 3 Mbps upload and download. The platform's technical support can help you test your speed before the first session.
- Private space: A quiet, well-lit room where you won't be overheard. Therapists often advise using headphones and a secure Wi-Fi network, not public hotspots.
Payment and Insurance: What to Expect
Many commercial platforms charge a flat monthly subscription that covers a set number of live sessions and unlimited messaging. Independent telehealth practitioners more often bill per session at rates comparable to in-person care. Insurance coverage for online counseling expanded during the pandemic and has since become permanent with many major plans. Verify your benefits: you may owe a co-pay or need to meet an annual deductible. Some employers offer Employee Assistance Programs (EAPs) that include several free online therapy sessions. Sliding-scale fees are also common, especially through community mental health centers and private practitioners who reserve a portion of their caseload for reduced-rate clients.
If you are considering formal training to deliver these services, exploring a master's degree in counseling is a strong starting point. Practitioners interested in couples and family modalities may also look into a master's in marriage and family therapy online.
Video Vs. Phone Vs. Text-Based Therapy: How Modalities Compare
An 850-adult randomized controlled trial published in JAMA Network Open found that message-based therapy produced depression outcomes comparable to video-based therapy over 12 weeks, a finding that challenges the assumption that live, face-to-face interaction is always necessary for clinical progress.1
Video-Based Therapy
Video sessions most closely resemble traditional in-person appointments. Multiple meta-analyses through 2024 report no significant difference in therapeutic alliance when comparing video to in-person delivery, and outcomes for anxiety, depression, and stress are broadly comparable.2 The main limitation is scheduling: the requirement to coordinate a synchronous session at a fixed time appears to contribute to slightly higher early dropout rates than asynchronous alternatives.3 For conditions requiring real-time clinical observation or frequent check-ins, video remains the most versatile format across a broad range of presenting concerns.
Phone-Based Therapy
Phone remains a practical option for clients who lack reliable internet access, prefer audio-only contact, or are not comfortable on camera. When sessions are structured and therapist-led, therapeutic alliance is reported to be comparable to other modalities.4 The evidence base here carries a notable caveat: phone calls are frequently grouped with video calls in research datasets rather than studied independently, which makes it difficult to draw firm conclusions about phone-specific outcomes. Dedicated head-to-head trials comparing phone to either text or video are still limited as of 2026.
Text and Message-Based Therapy
Asynchronous messaging is the format most distinct from conventional therapy. The Talkspace RCT referenced above found it non-inferior to video for depression treatment, and 2024 data suggest early dropout rates are actually lower for text-based modalities than for video.3 The working theory is that the low-friction, schedule-independent format sustains engagement for clients who would otherwise disengage before completing a course of care.
Therapeutic alliance in messaging therapy is harder to quantify. Standard alliance instruments were designed for live sessions, so most text-based alliance assessments are inferred from engagement patterns rather than validated scales, an acknowledged gap in the literature.1
Choosing a Format
No single modality suits every client or every presenting concern. Social workers pursuing clinical MSW programs will encounter these distinctions in their telehealth coursework. A practical framework:
- Video: Best for clients who benefit from visual cues, complex diagnoses, or structured weekly sessions.
- Phone: Best for clients with limited technology access or strong privacy concerns about video.
- Text-based: Best for clients needing schedule flexibility, those with communication anxiety, or situations where sustained engagement is a clinical priority.
Social workers building telehealth practices often offer more than one format, letting clinical judgment and client preference guide the match. Those interested in the broader landscape of mental health social work will find that modality selection is increasingly central to practice competency.
Is Online Counseling Effective? What the Research Says
One of the most common concerns about online counseling is whether it actually works as well as traditional, in-person therapy. The short answer: yes, for most people and most conditions, the outcomes are comparable.
A growing body of research spanning 2020 to 2026 consistently shows that online counseling produces results on par with face-to-face sessions.1 A systematic review published in 2024 examined 15 randomized controlled trials comparing online and in-person group psychotherapy. The findings revealed nonsignificant differences between the two formats, with both producing comparable outcomes.2 Only 3 of those studies favored in-person delivery, and just 2 met the most rigorous methodological standards, underscoring how much the field still needs high-quality research.
That said, the evidence is not uniformly positive across every condition and timeline. For depression specifically, telehealth counseling took approximately 12 weeks to reach clinical improvement, compared to roughly 8 weeks for in-person treatment.3 This gap matters. Clients dealing with severe depressive episodes may benefit from starting with face-to-face sessions when possible, then transitioning to online counseling for maintenance and ongoing support.
For practitioners exploring remote resources for mental health workers, understanding these nuances is essential. Effectiveness depends on several factors: the severity of the client's condition, the therapeutic modality being used, the quality of the technology platform, and the strength of the therapeutic alliance. Cognitive behavioral therapy (CBT), for example, translates particularly well to virtual formats because of its structured, goal-oriented design.
The bottom line for social workers considering telehealth practice is this: online counseling is a clinically sound option for the majority of clients, but it requires thoughtful assessment. Not every client or every condition is best served remotely. Knowing when to recommend in-person care, or a hybrid approach, is part of competent, ethical practice in the digital age.
Before the pandemic, just 2.1 percent of mental health visits among Medicare beneficiaries were conducted via telehealth. By 2024, that figure had risen to 42.9 percent, according to a five-year analysis published through the National Institutes of Health. That shift represents one of the fastest behavioral changes ever recorded in healthcare delivery.
Benefits and Drawbacks of Online Counseling
Online counseling offers meaningful advantages for both clients and practitioners, but it is not a perfect fit for every situation. Understanding these trade-offs helps social workers and prospective clients make informed decisions about whether telehealth modalities align with their needs.
Pros
- Eliminates geographic barriers, giving clients in rural or underserved areas access to licensed professionals they could not otherwise reach.
- Offers flexible scheduling, including evenings and weekends, which reduces missed appointments and supports clients with demanding work or caregiving responsibilities.
- Reduces overhead costs for practitioners, since there is no need to lease dedicated office space or maintain a physical waiting room.
- Clients who feel stigma around seeking therapy often find it easier to engage from the privacy of their own home.
- Provides continuity of care when clients relocate, travel, or face mobility challenges that make in-person visits difficult.
- Multiple modalities (video, phone, text) let practitioners tailor the format to each client's comfort level and clinical needs.
Cons
- Nonverbal cues such as posture, fidgeting, and subtle facial expressions are harder to read through a screen, potentially limiting clinical assessment.
- Technology issues, including poor internet connections, audio lag, or platform outages, can disrupt sessions and erode therapeutic rapport.
- Not clinically appropriate for clients in acute crisis, those with severe mental illness, or situations requiring immediate safety interventions.
- Licensing laws vary by state, requiring practitioners to hold credentials in every state where their clients are physically located during sessions.
- Maintaining HIPAA compliance demands ongoing investment in encrypted platforms, secure storage, and staff training on data privacy protocols.
- Some clients, particularly older adults or those with limited digital literacy, may struggle to navigate the technology required for virtual sessions.
Can Online Counselors Prescribe Medication?
Who Can Prescribe Medication?
Licensed clinical social workers (LCSWs), licensed professional counselors (LPCs), and marriage and family therapists (LMFTs) do not have prescribing authority; for a detailed look at how these professions differ, see social work vs counseling. Their training focuses on psychotherapy, behavioral interventions, and case management. Only psychiatrists (medical doctors) and psychiatric nurse practitioners (NPs) can prescribe psychiatric medications, including antidepressants, anti-anxiety agents, and mood stabilizers.2 In many states, primary care clinicians also prescribe basic psychiatric medications, but they often refer complex cases to a specialist.3 Telepsychiatry services now make it possible to see a prescriber remotely4, but controlled substances like stimulants for ADHD or certain anti-anxiety medications may have additional telehealth restrictions depending on state and federal regulations.5
Integrated Psychiatry Services on Online Platforms
Many online counseling platforms now offer integrated psychiatry services.6 Clients can continue seeing their therapist on the same platform while also scheduling separate medication evaluation and management sessions with a psychiatrist or psychiatric NP. This coordination streamlines care, but the roles are distinct: the counselor provides talk therapy, and the prescriber manages medication. Your therapist cannot write or refill a prescription, even within these integrated systems.
How to Find a Prescriber If You Need Medication
If you and your counselor determine that medication might help, several paths are available. Ask your therapist for a referral to a trusted psychiatric provider, either locally or online. Search for reputable telepsychiatry platforms that match you with a licensed prescriber in your state. You can also consult your primary care doctor, who may be comfortable starting you on a low dose or can direct you to a specialist. Always verify that any online prescriber requires a thorough initial assessment and ongoing monitoring, not just a brief questionnaire.
Therapy With or Without Medication
Many individuals benefit from counseling alone, especially when addressing adjustment challenges, relationship issues, or mild to moderate anxiety. For conditions like major depression, bipolar disorder, PTSD, or OCD, research consistently shows that combining therapy with medication is often more effective than either treatment alone. Your counselor can help you weigh the pros and cons and support you whether you choose to pursue medication or not. The goal is a care plan that fits your unique needs, with the understanding that counselors focus on therapeutic skills and emotional support while prescribers handle the medical aspects.
Privacy, Security, and HIPAA Compliance in Online Counseling
Delivering counseling online introduces real privacy obligations that differ from in-person practice. Understanding those obligations protects clients and keeps practitioners on the right side of federal law.
Core HIPAA Requirements for Online Counseling
The Health Insurance Portability and Accountability Act treats electronically transmitted protected health information (PHI) with the same seriousness as paper records. For online counseling, that translates into four concrete requirements.
- End-to-end encryption: Any video, audio, or text transmission containing PHI must be encrypted in transit so that intercepted data cannot be read.
- Business Associate Agreement (BAA): Before using any third-party platform to conduct or store sessions, the provider must sign a BAA with that vendor. The BAA formalizes the vendor's responsibility to safeguard PHI.
- Secure data storage: Session notes, recordings, and intake forms must be stored on servers that meet HIPAA security standards, including access controls and physical safeguards.
- Audit controls: Covered entities must maintain logs showing who accessed PHI and when, enabling investigation if a breach occurs.
Choosing a Compliant Platform
Not all video tools are built for clinical use. Consumer-grade applications designed for social or business communication typically do not offer BAAs and may route data through servers without healthcare-grade protections. Purpose-built telehealth platforms, by contrast, are engineered around HIPAA requirements from the start and will provide a BAA upon request. Practitioners, including those building a private practice social work caseload, should treat the willingness to sign a BAA as a baseline, non-negotiable criterion when evaluating any platform.
What Clients Should Verify Before a First Session
Clients carry some responsibility for their own privacy as well. Before meeting with a counselor online, it is reasonable to ask:
- Whether the platform uses encryption and can provide documentation of its security practices
- What the provider's data retention policy covers and how long session records are kept
- Whether sessions are ever recorded, and if so, who controls access to those recordings
- Where the privacy policy is published and how to file a complaint if privacy rights are violated
The Post-COVID Regulatory Landscape
During the COVID-19 public health emergency, the Department of Health and Human Services exercised enforcement discretion that allowed providers to use non-HIPAA-compliant communication tools for telehealth in good faith. That flexibility expired when the federal public health emergency ended in May 2023. For a broader look at how the pandemic reshaped the profession, see this COVID-19 guide for social workers. As of 2026, providers must use fully compliant platforms, sign BAAs, and meet all standard HIPAA requirements without exception. One meaningful flexibility that has survived the emergency period is the continued allowance for many practitioners to deliver telehealth services across state lines under temporary interstate licensure compacts, though those rules vary by state and profession and are separate from HIPAA itself.
Questions to Ask Yourself
When Online Counseling Is Not Appropriate
Telehealth has become a default delivery method for outpatient mental health, but clinical consensus from NASW, ACA, and APA is clear that certain presentations require in-person care or coordinated crisis response.12 Knowing where the modality fails is as important as knowing where it works.
Clinical Scenarios Where Telehealth Is Contraindicated
Online counseling is generally not appropriate, or is only appropriate with significant safeguards, in the following situations:
- Active suicidality or homicidal ideation with means and intent: Risk that requires immediate physical intervention exceeds what a video screen can provide.
- Acute psychosis: Disorganized thought and impaired reality testing make remote rapport and assessment unreliable.
- Severe substance intoxication or withdrawal: Medical stabilization, not therapy, is the first need. Practitioners who specialize in this area, such as substance abuse social workers, often coordinate with emergency departments before any telehealth follow-up begins.
- Intimate partner violence where a partner may overhear: A session conducted in a shared home can escalate danger rather than reduce it.
- Severe cognitive impairment: Clients who cannot operate the technology, recall session content, or provide informed consent are poorly served by a remote format.
Crisis Protocol During a Telehealth Session
Ethical guidelines require clinicians to prepare before a crisis happens, not during one. Before treatment begins, verify the client's physical location, document an emergency contact, identify local crisis resources, obtain consent, and discuss the limits of confidentiality early.1 At the start of each session, re-confirm location and whether the client is alone.4 If location changes mid-care or risk escalates, re-verify immediately.4
When risk surfaces during a session, complete a structured risk assessment, determine whether the client is safe, and decide between continued support and emergency dispatch.5 If imminent danger is present, stay on the line, direct the client toward emergency care, contact local emergency services, and notify the documented emergency contact. If the call disconnects, use the emergency contact to attempt follow-up and request a welfare check.1 Document the risk assessment, actions taken, consultations, disclosures, and follow-up plan in the clinical record. Mandatory reporting obligations are governed by the state where the client is physically located.1
Special Populations
Minors require guardian consent and a private space at home, which is not always available. Older adults may face technology and sensory barriers that warrant in-person or hybrid care; understanding the broader challenges of reducing social isolation in older adults can help practitioners decide when telehealth alone is insufficient. For any client with severe cognitive impairment, confirm that a caregiver can support the session or refer to in-person services.
A Simple Decision Framework
- If a client presents with active suicidality, psychosis, intoxication, or unsafe home conditions, refer to in-person or crisis services (988, local mobile crisis teams, emergency departments).6
- If a client has moderate symptoms, a stable environment, reliable technology, and a documented safety plan covering warning signs, coping steps, escalation criteria, a local emergency number, a backup phone number, and an emergency support person, online counseling can work with appropriate safeguards.1
Telehealth Social Work: Career Outlook and Salary
The Bureau of Labor Statistics groups many telehealth counseling roles under the broader occupation of Substance Abuse, Behavioral Disorder, and Mental Health Counselors (SOC 21-1018). The figures below reflect national wage data from the BLS (approximately 2024) for this full occupation, not exclusively telehealth positions. Because the CIP-to-SOC crosswalk maps multiple degree programs to this single occupation code, salaries for practitioners who work primarily via telehealth may differ from these benchmarks. With a projected job growth rate of 17% from 2024 to 2034 and roughly 48,300 annual openings, demand in this field is well above the average for all occupations.
| Metric | National Figure |
|---|---|
| Total Employment | 440,380 |
| Annual Median Wage | $59,190 |
| 25th Percentile Wage | $47,170 |
| 75th Percentile Wage | $76,230 |
| Mean (Average) Wage | $65,100 |
| Projected Growth (2024 to 2034) | 17% |
| Estimated Annual Openings (2024 to 2034) | 48,300 |
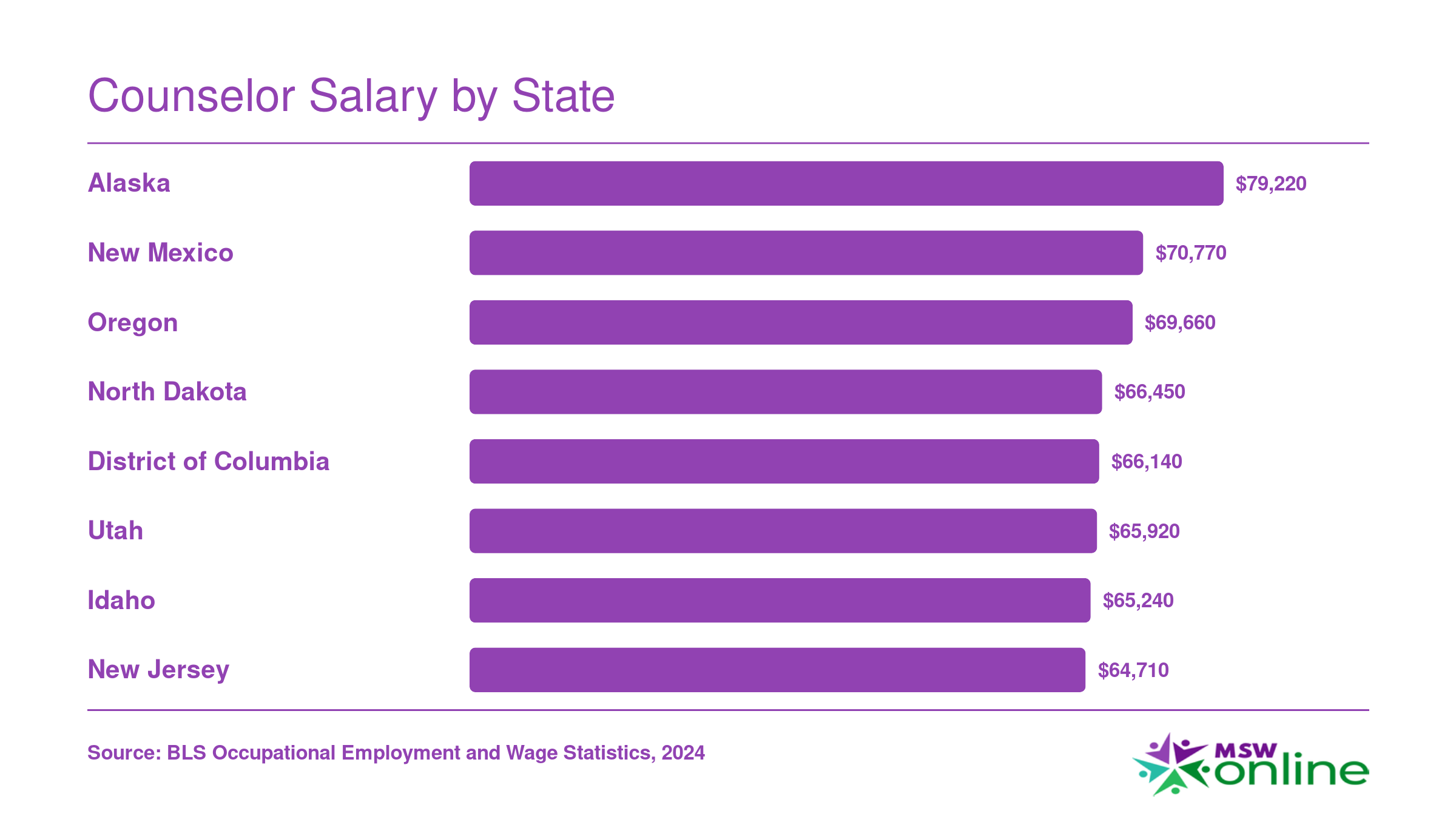
Counselor Salary by State
Compensation for substance abuse, behavioral disorder, and mental health counselors varies significantly across the country. States with higher costs of living, stricter licensure requirements, or acute workforce shortages tend to offer the highest median salaries. Below are the top eight highest-paying states by annual median wage.
How Social Workers Can Start an Online Counseling Practice
Forty states plus DC have now joined the Counseling Compact, but only four jurisdictions (Arizona, Minnesota, Ohio, and Louisiana) were actually issuing compact privileges as of April 2026.1 That gap between membership and operational status shapes everything about how clinicians launch a telehealth practice today: where you can see clients, how you market, and which licenses you need to maintain.
Step 1: Lock Down Licensure and Jurisdiction
Start with the credential. For social workers, that means the LCSW (or state equivalent); for counselors, the LPC; for marriage and family therapists, the LMFT. Full clinical licensure is non-negotiable for independent practice and insurance paneling.
Next, map your jurisdictional footprint. The governing standard is that you practice where the client is located, not where you sit, and that location must authorize you to provide care.1 In non-compact states and in large markets like California, New York, and Massachusetts, that means holding a full in-state license for every state where you intend to see clients via telehealth. If you are an LPC in an operational compact state, the Counseling Compact privilege lets you treat clients in other operational states without a separate license, with 35 states still completing implementation and Nevada's law taking effect January 2026.2 Social workers do not yet have an equivalent. The ASWB-backed Social Work Licensure Compact is in an earlier adoption phase, so LCSWs should expect to pursue licensure state by state for now.1
Step 2: Build the Operational Stack
- Platform: Choose a HIPAA-compliant video and documentation system with a signed business associate agreement. Consumer Zoom and SMS do not qualify.
- Niche: Specialize. Trauma, perinatal mental health, LGBTQ+ affirming care, addiction, and chronic illness all draw steady referrals and justify premium self-pay rates. Trauma certifications for social workers can strengthen credibility and open referral pipelines in high-demand specialties.
- Billing and paneling: Decide between cash-pay, in-network panels, or a hybrid. Insurance credentialing typically takes 90 to 120 days per payer.
Step 3: Marketing and Referrals
List on Psychology Today, TherapyDen, Inclusive Therapists, and any directories tied to your niche. Build a simple website optimized for local search terms ("online therapist [city]" still converts), and cultivate referral relationships with primary care physicians, psychiatrists, and school counselors in the states where you are licensed.
Step 4: Protect Yourself From Screen Burnout
Back-to-back video sessions produce a distinct fatigue: reduced nonverbal feedback, constant self-view, and zero physical transitions between clients. Cap your clinical hours below what you would carry in person (many telehealth clinicians settle around 20 to 25 sessions weekly), build 15-minute buffers between appointments, schedule camera-off administrative blocks, and maintain your own consultation group. Sustainable practice is part of the business model, not an afterthought.
Frequently Asked Questions About Online Counseling
Online counseling raises practical questions about effectiveness, insurance, privacy, and logistics. Below are concise answers to the concerns prospective clients and practitioners ask most often.