Points of interest…
- Burnout prevalence among U.S. social workers reached 57% by 2026, with emotional exhaustion rates hitting 70%.
- CMS has made several pandemic-era telehealth flexibilities permanent, though state licensure rules still vary widely.
- Roughly 5.3% of U.S. adults reported long COVID symptoms as of 2024 to 2025, creating sustained demand for social work services.
- Nearly 60% of licensed clinical social workers now receive some or all supervision virtually, per a 2023 CSWA survey.
A Social Worker's Guide to COVID-19: What You Need to Know in 2026
The COVID-19 pandemic permanently reshaped social work practice, from service delivery models and ethical frameworks to workforce well-being and career trajectories. This guide consolidates what social workers need to know in 2026: how telehealth regulations have settled, which ethical decision-making frameworks hold up under crisis conditions, how to support clients living with long COVID, and what the evidence says about burnout, moral injury, and organizational responsibility. Whether you are exploring careers in social work or already managing a caseload, each section offers actionable protocols, validated tools, and direct links to authoritative sources so you can practice effectively in a profession that the pandemic changed for good.
How COVID-19 Transformed Social Work Practice
The COVID-19 pandemic reshaped nearly every aspect of social work, forcing practitioners to adapt rapidly to new service delivery models, heightened client needs, and unprecedented ethical challenges. Understanding these shifts is essential for any social worker navigating the post-pandemic landscape.
One of the most visible changes was the widespread adoption of telehealth and virtual casework. Before the pandemic, most social workers conducted sessions and home visits in person. Lockdowns and safety protocols made that impossible almost overnight, pushing agencies to embrace video conferencing, phone check-ins, and digital documentation systems. While telehealth expanded access for some clients, it also exposed deep inequities: many vulnerable populations lacked reliable internet, devices, or private spaces for confidential conversations.
Client needs intensified across virtually every population. Job losses, housing instability, food insecurity, and domestic violence surged during lockdowns. Mental health crises spiked as isolation, grief, and uncertainty took a toll on individuals and families. Practitioners working with older adults saw firsthand how pandemic restrictions amplified loneliness and depression, a challenge explored in depth in strategies to combat loneliness in elderly populations. Meanwhile, substance abuse social workers reported sharp increases in relapse and overdose cases tied to disrupted treatment access and pandemic-related stress.
Workforce strain became a defining issue as well. Social workers faced higher caseloads, compassion fatigue, and their own health anxieties, all while navigating shifting public health guidelines. Many practitioners pursued accelerated social work programs online to gain new credentials and stay competitive in an evolving field.
The pandemic also forced the profession to confront systemic disparities more directly. Communities of color and low-income populations bore disproportionate health and economic burdens, reinforcing calls for anti-racist, equity-centered practice. Professional organizations updated ethical guidelines to address remote service delivery, informed consent in digital settings, and the duty to protect both clients and practitioners.
These transformations were not temporary. Hybrid service models, telehealth competencies, and a sharper focus on health equity remain central to social work practice today.
Ethical Decision-Making Frameworks for Pandemic Conditions
Ethical decision-making in pandemic conditions means choosing the best possible course of action when the rules you normally follow, the resources you normally have, and the client relationships you normally maintain are all under strain at the same time. Social workers confronted these dilemmas at scale during COVID-19, and the frameworks that emerged continue to shape practice in 2026.
Why Standard Ethics Codes Are Not Enough on Their Own
The NASW Code of Ethics remains the bedrock of professional conduct, but it was designed for stable practice environments. Pandemics introduce competing obligations: duty to individual clients versus duty to community health, the imperative to maintain confidentiality versus public health reporting mandates, and the tension between client self-determination and infection-control directives. When you face a triage scenario where two clients need the same scarce resource, the Code alone does not tell you who to prioritize. That is where supplemental frameworks come in.
The NASW, the Council on Social Work Education (CSWE), and the International Federation of Social Workers (IFSW) all published guidance documents in the pandemic's wake that address exactly these gaps. If you have not reviewed them recently, go directly to each organization's website and search their standards and publications libraries. These documents are updated periodically, and the versions posted in 2024 and 2025 reflect lessons learned rather than emergency improvisation.
A Practical Process for Working Through Dilemmas
Rather than memorizing every position paper, build a repeatable process you can apply under pressure. The following steps synthesize recommendations from multiple professional bodies:
- Identify the competing obligations. Name each stakeholder and what you owe them: client autonomy, public safety, employer directives, community welfare.
- Consult the most current guidance. Check NASW's practice standards page, CSWE's educational policy statements, and your state licensing board's pandemic-specific advisories. Guidance varies by jurisdiction.
- Assess proportionality. Ask whether the restriction you are considering (for example, requiring telehealth instead of in-person sessions) is proportional to the actual risk. Outdated protocols can harm clients unnecessarily.
- Document your reasoning. Record the ethical principles you weighed, the sources you consulted, and the rationale for your final decision. Documentation protects both you and your client.
- Seek consultation. Use peer consultation, supervision, or your agency's ethics committee before acting on high-stakes decisions whenever possible.
Where to Find Authoritative, Up-to-Date Information
Practitioners sometimes struggle not with the willingness to follow ethical guidance but with locating the right documents. A few direct pointers:
- The NASW website hosts its Code of Ethics, supplemental practice standards, and policy statements under clearly labeled menus. Search for pandemic-related advisories by keyword.
- CSWE publishes educational policy and accreditation standards that inform how ethics are taught; these shape the competencies you are expected to demonstrate in practice.
- The IFSW maintains a global ethics statement and has published position papers on social work during health emergencies. These are especially useful if you work with international populations or in international social work.
- Your state licensing board may have issued emergency rules during COVID-19, some of which have been made permanent. Check the board's website directly rather than relying on secondhand summaries.
- For salary benchmarks and labor market data that inform resource-allocation decisions at an organizational level, the Bureau of Labor Statistics (bls.gov) provides occupation-specific wage data updated annually.
Dual Loyalty and Ongoing Vigilance
One concept that gained traction during the pandemic is dual loyalty, the conflict that arises when your employer's interests diverge from your client's needs. An agency might push for rapid case closures to manage volume while a client's situation demands sustained engagement. Recognizing dual loyalty as an ethical category, not just a workplace frustration, helps you name the problem and address it through proper channels such as supervision, union representation, or ethics consultation. Holding relevant certifications for social workers can also strengthen your standing when advocating through these channels.
Ethical frameworks are living tools. Revisit them regularly, especially as pandemic-era emergency orders expire and practice norms continue to shift. The goal is not perfect certainty; it is a defensible, transparent process that centers client welfare even when conditions are far from ideal.
Questions to Ask Yourself
Telehealth Best Practices for Social Workers
Which pandemic telehealth flexibilities are still in effect in 2026, and which ones have expired? The answer matters for billing, licensure, and how you structure your practice going forward.
The Current Regulatory Landscape
CMS has cemented several pandemic-era flexibilities while letting others lapse.1 For Medicare behavioral health services, clinical social workers remain permanent eligible distant-site providers, audio-only sessions for behavioral health are permanently reimbursable, and the patient's home is a permanent originating site.2 Providers can also deliver care from their own home without enrolling that home address. One catch worth noting: behavioral health telehealth requires an in-person visit within six months prior to the initial telehealth encounter and annually thereafter, though the annual requirement can be waived with clinical documentation.1
For non-behavioral telehealth services, the broader audio-only allowance and expanded originating-site rules have been extended only through December 31, 2027, per the latest CMS guidance.1 At the state level, many Medicaid programs and commercial payers have made the home as an originating site and audio-only behavioral health coverage permanent, though specifics vary widely.3 NASW and CCHPCA both maintain updated trackers worth bookmarking.
Evidence-Based Practice Standards
Four practices should anchor your telehealth workflow:
- Structured session openings: Confirm location, verify a private space, identify a support contact, and review the emergency plan before clinical content begins. This compensates for the lost contextual cues of an in-person visit.
- Validated remote risk-assessment tools: Use instruments adapted or validated for telehealth, such as the Columbia Suicide Severity Rating Scale (C-SSRS), and document collateral contacts and local emergency resources for each client.
- HIPAA-compliant platforms: The pandemic-era enforcement discretion for consumer platforms ended in 2023. Use a vendor offering a signed BAA, end-to-end encryption, and audit logging. Standard FaceTime, Zoom (non-healthcare tier), and SMS no longer meet the bar.
- Hybrid scheduling: Build in-person checkpoints into otherwise virtual caseloads, especially around intakes, safety planning, and treatment plan reviews.
When to Default to In-Person
A simple decision tree helps: if a client presents with active suicidal ideation, severe dissociation, recent psychiatric hospitalization, or domestic violence safety concerns, default to in-person. If the client has stable symptoms, prefers telehealth, and has reliable private technology access, default to virtual. Mixed signals (moderate acuity, technology barriers, ambivalent client preference) point to a hybrid rhythm with monthly or quarterly in-person sessions. Social workers building or expanding a telehealth caseload may also want to explore private practice social work models that integrate virtual and in-person service delivery.
Cross-State Practice and the ASWB Compact
The federal cross-state telehealth waiver has expired, so practicing across state lines now depends on individual state rules.4 Some states offer telehealth-specific registration for out-of-state social workers.3 The ASWB Social Work Licensure Compact has been enacted in a substantial number of states but is not yet fully operational, meaning the privilege-to-practice mechanism is not live for clinicians.3 Until it launches, hold a license in every state where your clients are physically located during sessions, and check state board guidance before accepting an out-of-state referral.
Supporting Clients With Long COVID
Two approaches dominate long COVID care: a narrow medical lens that chases isolated symptoms, and a comprehensive functional framework that addresses the whole person. Social workers are uniquely positioned to lead the latter, not by treating the virus, but by restoring daily life.
Defining Long COVID Through a Functional Lens
Long COVID is not a single diagnosis but a constellation of persistent symptoms lasting three months or more after initial infection. For social workers, the focus belongs on functional impairment, not virology. An estimated 6 to 7% of U.S. adults have experienced long COVID symptoms that significantly interfere with daily activities: cognitive fog that derails work performance, fatigue that prevents basic self-care, pain that isolates from social connection. The Post-COVID Functional Status scale (PCFS) captures this reality with an ordinal scale ranging from no limitation to severe dependency, grounding the clinical picture in what clients can or cannot do.2
Cognitive impairment often overshadows other symptoms. Traditional screens like the MoCA miss subtle executive dysfunction. The PROMIS Cognitive Function Short Form 8a, validated in 2024, outperforms the MoCA at predicting real-world functional decline. Combined with the Everyday Cognition scale (ECog-2), these tools help social workers pinpoint where a client is struggling, whether that means managing finances, keeping appointments, or following treatment plans.4
A Practical Assessment Framework
Social workers need a structured yet flexible assessment that goes beyond a medical checklist. Begin with functional screening: - Cognitive: Can the client manage their medication schedule, complete work tasks, or follow a conversation? Use PROMIS Cognitive Function and ECog-2. - Physical: What daily activities are limited by fatigue, pain, or breathlessness? The PROMIS Physical Function and Fatigue scales quantify these losses. - Overall status: The PCFS provides a snapshot of post-COVID functional dependency.
Next, screen for mental health comorbidities. Depression and anxiety are common, often exacerbated by the uncertainty of long COVID. Practitioners who specialize in social work in mental health routinely use the PHQ-9 and GAD-7 as quick, validated measures. For clients with traumatic illness experiences, a brief PTSD screen may also be warranted.
Finally, map social determinants. Long COVID disproportionately deepens existing vulnerabilities: job loss, housing instability, and food insecurity. Ask directly about employment status, eviction risk, and access to benefits. A recommended assessment battery combines PROMIS Cognitive Function, Physical Function, Fatigue, PCFS, ECog-2, PHQ-9, and GAD-7, a suite that captures functional, emotional, and social dimensions without overwhelming the client.2
Navigating Disability Benefits and Workplace Rights
Many clients with long COVID qualify for disability protections. In 2021, the U.S. Department of Health and Human Services and Department of Justice recognized long COVID as a disability under the Americans with Disabilities Act (ADA). A disability social worker can guide clients through this bureaucracy by documenting how symptoms substantially limit major life activities, using functional assessment tools as evidence. For Social Security Disability Insurance (SSDI) or Supplemental Security Income (SSI), detailed records of functional limitations, failed work attempts, and medical treatments are critical.
Workplace accommodations under the ADA might include flexible schedules, remote work, cognitive support tools, or ergonomic adjustments. Social workers coach clients on how to request these accommodations and navigate Family and Medical Leave Act (FMLA) protections for intermittent leave during flare-ups. Advocacy often means educating employers that long COVID is not a matter of "pushing through" but a fluctuating, disabling condition.
The Interdisciplinary Care Coordination Model
Long COVID demands a team, and the social worker is the linchpin. Interdisciplinary long COVID clinics bring together primary care physicians, pulmonologists, neuropsychologists, occupational therapists, and behavioral health specialists.2 The social worker's role is to translate clinical findings into real-world adaptations, communicating functional goals back to the team, linking clients to community resources, and addressing the social determinants that undermine recovery.
In settings without a formal clinic, social workers still coordinate. They facilitate warm handoffs to neuropsychology for cognitive rehabilitation (such as the BrainHQ or PASC-CoRE interventions studied in 2024 trials), ensure occupational therapy addresses energy conservation and daily living skills, and bridge gaps between medical and social systems.4 This model prevents fragmentation and reinforces that long COVID is not merely a medical puzzle but a life-disrupting event.
Resources for Clients and Practitioners
- Clinic directories: Survivor Corps maintains a searchable map of post-COVID care centers across the U.S.; many academic medical centers list their long COVID programs online.
- Patient advocacy organizations: Body Politic and Survivor Corps provide education, peer connection, and policy advocacy. The COVID-19 Longhauler Advocacy Project offers guidance on disability applications.
- Peer support groups: Online communities like the Long COVID Support Facebook group or local meetups offer emotional validation and practical strategies. Referring clients to these groups reduces isolation and builds collective knowledge.
According to the CDC, roughly 5.3% of U.S. adults reported experiencing long COVID as of 2024 to 2025. That translates to millions of people navigating persistent symptoms, and researchers estimate the condition has pushed a meaningful share of affected individuals out of the workforce entirely, with ripple effects on disability applications and household economic stability.
Remote Supervision and Organizational Supports
A 2023 survey by the Clinical Social Work Association found that nearly 60 percent of licensed clinical social workers reported receiving some or all of their supervision virtually, a shift that persisted well beyond initial lockdowns. That statistic reflects a permanent change in how the profession cultivates reflective practice, and it demands deliberate adaptation from both supervisors and the organizations that employ them.
Why Supervision Needed Reinvention
Traditional supervision relied on proximity. A quick hallway check-in after a difficult intake, a supervisor noticing a clinician's slumped posture before a team meeting, the organic rhythm of shared office space: all of these informal touchpoints fed reflective practice without anyone scheduling them. Video platforms stripped most of that away. Supervisors lost the ability to read subtle nonverbal cues, and supervisees lost the casual peer contact that normalizes emotional reactions to heavy caseloads. The result was isolation that, left unchecked, eroded both clinical growth and professional resilience.
Concrete Adaptations Agencies Have Adopted
Organizations that navigated the transition successfully moved beyond simply replicating an in-person hour on Zoom. Common adaptations include:
- Structured virtual check-ins with dedicated reflective time: Rather than cramming administrative updates and clinical review into a single call, agencies now split sessions so that at least half the supervision hour is reserved for processing emotional responses and exploring practice dilemmas.
- Asynchronous case consultation platforms: Secure messaging boards or HIPAA-compliant shared workspaces let clinicians post de-identified case questions and receive peer and supervisor feedback outside of scheduled meetings, partially replacing the hallway consult.
- Peer-support dyads: Pairing supervisees for weekly co-reflection gives each clinician a consistent sounding board, reducing dependence on a single supervisor and strengthening lateral trust.
- Hybrid supervision schedules: Many agencies now rotate in-person supervision days so that each supervisee has at least one face-to-face session per month, preserving the nonverbal richness that video cannot fully replicate.
Maintaining Team Cohesion Remotely
Supervision happens within an organizational culture, and culture erodes quickly without intentional upkeep. Agencies that report high staff retention have adopted virtual team rituals: brief Monday morning stand-ups focused on morale rather than metrics, shared case-review meetings where multiple disciplines contribute, and rotating in-person days designed less for productivity and more for reconnection. These practices keep practitioners feeling like members of a team rather than isolated contractors, whether they work in child social worker roles or across other specializations.
Monitoring Vicarious Trauma in Remote Staff
Supervisors carry an ethical obligation that intensifies in a remote environment. Without physical co-presence, signs of vicarious trauma or moral injury are easier to miss. Proactive screening matters: brief validated measures at regular intervals, direct questions about sleep and emotional load, and explicit invitations to discuss distress. The NASW Code of Ethics places responsibility on supervisors to safeguard the well-being of those they oversee. Waiting for a supervisee to self-report burnout over a video call is not sufficient. Supervisors must build check-in protocols that surface problems before they become crises, and organizations must give supervisors the time, training, and structural support to do so consistently. Practitioners considering a licensed clinical social worker private practice model face these supervision challenges in an even more acute form, since they may lack built-in organizational supports entirely.
Setting-Specific Practice Protocols
Social work practice settings each carry distinct pandemic-related challenges that require tailored protocols. The table below outlines key adaptations, risk factors, and current best practices across major practice environments as of 2026. Settings that moved aggressively toward hybrid models early in the pandemic have generally retained those structures, while others have returned to predominantly in-person service delivery with enhanced safety measures.
| Practice Setting | Key Pandemic Adaptations | Risk Considerations | Current Best Practice (2026) |
|---|---|---|---|
| Hospital / Medical Social Work | Shifted to telehealth for discharge planning when possible; adopted PPE protocols for in-person contact; embedded in interdisciplinary COVID response teams | High exposure risk in acute care units; moral distress from resource scarcity and triage decisions; secondary traumatic stress from patient deaths | Hybrid discharge planning combining in-person assessment with virtual family conferences; ongoing infection control training; routine mental health check-ins for staff |
| School Social Work | Transitioned to virtual counseling during closures; developed remote wellness checks and crisis protocols for students at home | Difficulty identifying abuse or neglect without in-person observation; increased student mental health needs; technology access gaps among low-income families | In-person services restored with telehealth as a supplement for homebound or quarantined students; strengthened partnerships with community mental health providers; trauma-informed classroom consultation |
| Child Welfare / Child Protective Services | Adopted virtual home visits when in-person access was restricted; created safety assessment tools for remote use; modified court hearing procedures | Reduced ability to observe living conditions and detect maltreatment remotely; case backlog during lockdowns; worker safety during home visits in high-transmission periods | In-person home visits as the standard, with virtual follow-ups permitted for lower-risk cases; updated safety assessment protocols that account for pandemic-related family stressors; caseload management reforms |
| Community Mental Health | Rapid expansion of telehealth therapy and group sessions; crisis hotline staffing increases; integration of COVID-specific psychoeducation into treatment plans | Client digital literacy barriers; confidentiality concerns in shared living spaces; increased demand for services outpacing provider capacity | Sustained telehealth option alongside in-person sessions (client choice model); long COVID screening integrated into intake assessments; waitlist management through stepped-care frameworks |
| Substance Use Treatment | Shifted group programming to virtual formats; adopted federal flexibilities allowing take-home medications (e.g., methadone); expanded peer support via phone and text | Isolation increased relapse risk; reduced access to mutual aid meetings; overdose deaths spiked during pandemic waves | Retention of expanded take-home medication policies where clinically appropriate; hybrid group therapy models; naloxone distribution integrated into all intake and discharge protocols |
| Aging and Geriatric Services | Implemented remote wellness checks and meal delivery coordination; facilitated virtual family visits in long-term care; advocated for resident rights during facility lockdowns | Social isolation contributing to cognitive decline and depression among older adults; high COVID mortality in congregate settings; caregiver burnout | Person-centered visiting policies that balance infection control with psychosocial needs; technology access programs for older adults; routine loneliness and depression screening at every contact |
| Private Practice | Full transition to telehealth during early pandemic; navigated evolving insurance reimbursement for virtual sessions; adjusted informed consent and confidentiality procedures | Blurred work-life boundaries for practitioners; screen fatigue for both clinician and client; liability questions around cross-state telehealth | Clear telehealth policies in informed consent documents; compliance with state-specific interstate practice compacts; structured self-care plans to address clinician burnout |
Burnout, Moral Injury, and Self-Care Strategies
Burnout is now the default state of the social work workforce, not an outlier condition affecting a stressed minority. National data from 2026 puts burnout prevalence among U.S. social workers at 57%, with emotional exhaustion reaching 70%.1 Pre-pandemic baselines hovered closer to 30-40% depending on setting. Child welfare social workers are hit hardest at 69%, followed by healthcare social workers at 65% and elderly care workers at 61%. Turnover intentions have climbed: roughly 27% of social workers report increased intent to leave the profession because of burnout, and child welfare turnover is running at 30-40% annually in many jurisdictions.2
Burnout Is Not Moral Injury
These are related but distinct conditions, and conflating them leads to the wrong interventions. Burnout is the cumulative exhaustion, cynicism, and reduced efficacy that follows chronic workplace stress. It responds, at least partially, to rest, workload adjustment, and recovery.
Moral injury is different. It is the lasting psychological, social, and spiritual harm that comes from being forced to act, or witness others act, in ways that violate your professional ethics. For social workers, this looked like denying services to clients who clearly needed them, discharging hospital patients to unsafe housing because no beds existed, watching child welfare cases close without resolution because caseloads were unmanageable, or being unable to honor informed consent because telehealth platforms were imposed overnight. You cannot vacation your way out of moral injury. It requires processing the ethical wound itself, often through structured reflection, peer dialogue, or trauma-focused therapy.
Individual Strategies That Actually Help
- Self-assessment with validated tools: The Professional Quality of Life Scale (ProQOL) measures compassion satisfaction, burnout, and secondary traumatic stress separately. Use it quarterly to track which dimension is shifting.
- Structured peer consultation: Peer support groups show a 22% reduction in burnout symptoms. Reflective supervision, when available, shows 27%.1
- Boundary practices: Hard stops on after-hours messaging, caseload caps you communicate in writing, and explicit scope-of-practice language with referral sources.
- Trauma-informed self-care: This means addressing the nervous system, not buying bath bombs. Mindfulness training shows 30% burnout reduction; resilience training shows 40%.1 SAMHSA's Disaster Behavioral Health resources offer free, evidence-informed protocols.
The Organizational Side
Individual strategies cap out fast when the system itself is the problem. The most effective interventions are structural: caseload reduction shows a 35% burnout reduction, wellness initiatives 45%, and flexible work arrangements 28%.1 Agencies that frame burnout as a personal resilience failure are misreading the evidence and shifting liability onto the workers least able to fix it.
Pandemic-Era Burnout at a Glance
The COVID-19 pandemic intensified existing stressors across the social work profession. These figures capture the scope of burnout and moral injury that reshaped workforce dynamics during and after the pandemic.
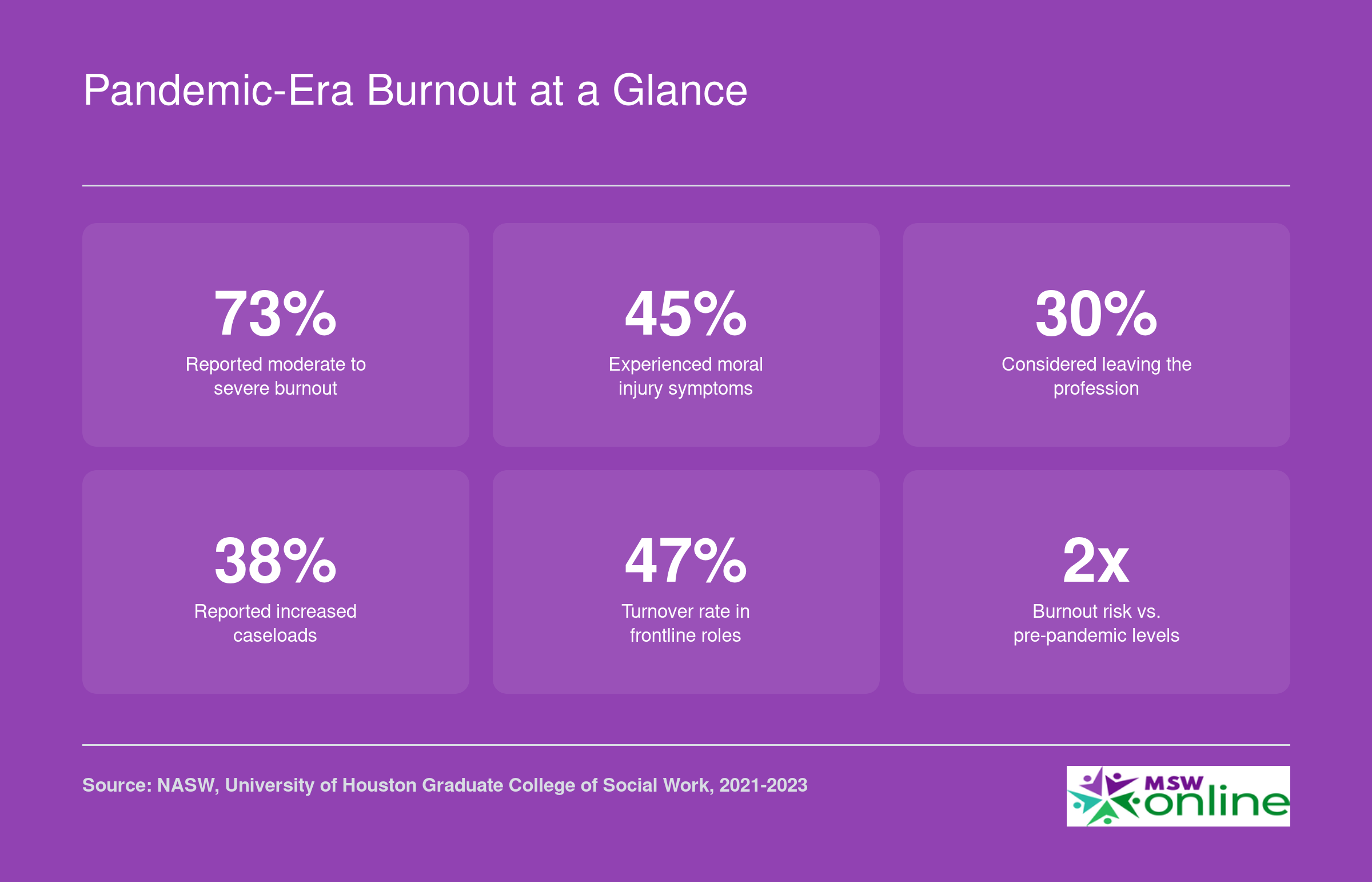
Burnout is not a personal failing, and agencies that treat it as one make the problem worse. Research consistently shows that structural interventions, including manageable caseloads, reflective supervision, and hazard compensation, produce better outcomes than individual self-care mandates placed on workers who are already stretched thin.
Social Work Salary and Career Outlook After the Pandemic
The pandemic expanded demand for social workers across healthcare, schools, and community agencies, and that momentum continues. According to the Bureau of Labor Statistics, the broad Social Workers category (SOC 21-1020) employed nearly 760,000 professionals nationally as of the most recent data, with a projected job growth rate of 6 percent over the coming decade, faster than the all-occupations average. The table below breaks out national median and mean salaries, plus the 25th-to-75th percentile range, for the major social work occupation groups. These figures can help you benchmark where you stand now and where additional credentials or specialization could move you.
| Occupation | Total National Employment | National Median Salary | National Mean Salary | 25th Percentile | 75th Percentile |
|---|---|---|---|---|---|
| Social Workers (All, SOC 21-1020) | 759,740 | $61,330 | $67,050 | $48,680 | $78,500 |
| Child, Family, and School Social Workers | 382,960 | $58,570 | $62,920 | $47,480 | $74,060 |
| Healthcare Social Workers | 185,940 | $68,090 | $72,030 | $55,360 | $83,410 |
| Social Workers, All Other | 64,940 | $69,480 | $74,680 | $52,010 | $95,390 |
Social Worker Salaries by State
Salaries for social workers vary significantly by state, specialty, and setting. The table below draws from BLS state-level data across three occupation categories: healthcare social workers, child/family/school social workers, and all other social workers. Keep in mind that higher median wages in states like California, Connecticut, and the District of Columbia often coincide with elevated costs of living, which can reduce real purchasing power. Meanwhile, several states that expanded Medicaid or invested heavily in public health infrastructure during and after the pandemic, such as Washington, Oregon, and Minnesota, show robust employment numbers across multiple social work categories.
| State | Occupation | Total Employment | Median Annual Wage | 25th Percentile | 75th Percentile |
|---|---|---|---|---|---|
| California | Healthcare Social Workers | 19,680 | $92,970 | $67,880 | $122,200 |
| District of Columbia | Healthcare Social Workers | 490 | $92,600 | $77,790 | $105,750 |
| Oregon | Healthcare Social Workers | 2,050 | $85,150 | $66,650 | $102,390 |
| Hawaii | Healthcare Social Workers | 680 | $84,640 | $58,270 | $95,520 |
| Connecticut | Healthcare Social Workers | 2,010 | $81,900 | $73,200 | $97,140 |
| New Jersey | Healthcare Social Workers | 4,390 | $81,710 | $66,100 | $100,200 |
| Rhode Island | Healthcare Social Workers | 570 | $79,460 | $63,450 | $91,510 |
| Washington | Social Workers, All Other | 870 | $96,550 | $70,410 | $112,320 |
| Massachusetts | Social Workers, All Other | 590 | $94,000 | $72,880 | $112,650 |
| Georgia | Social Workers, All Other | 1,180 | $92,750 | $59,810 | $110,930 |
| South Carolina | Social Workers, All Other | 500 | $91,940 | $71,390 | $106,870 |
| Delaware | Social Workers, All Other | 140 | $91,710 | $63,400 | $106,580 |
| Connecticut | Child, Family, and School Social Workers | 5,360 | $78,940 | $63,730 | $98,060 |
| District of Columbia | Child, Family, and School Social Workers | 2,800 | $78,920 | $59,280 | $95,820 |
| New Jersey | Child, Family, and School Social Workers | 6,410 | $78,150 | $59,590 | $98,920 |
| Washington | Child, Family, and School Social Workers | 10,570 | $72,290 | $58,250 | $84,180 |
| California | Child, Family, and School Social Workers | 55,220 | $69,250 | $54,890 | $88,190 |
| New York | Child, Family, and School Social Workers | 27,220 | $65,430 | $57,950 | $82,980 |
| Minnesota | Healthcare Social Workers | 2,530 | $72,330 | $60,830 | $84,490 |
| Minnesota | Child, Family, and School Social Workers | 6,430 | $65,010 | $54,230 | $79,450 |
| Minnesota | Social Workers, All Other | 7,240 | $79,220 | $65,810 | $92,800 |
| Texas | Social Workers, All Other | 2,700 | $89,520 | $53,200 | $113,840 |
Frequently Asked Questions About COVID-19 and Social Work
The pandemic reshaped virtually every corner of the profession, and many of those changes are still evolving. Below are concise answers to the questions social workers ask most often, along with frameworks and resources you can consult for deeper guidance.
Explore More
- Bilingual Social Worker
- Continuing Education for Social Workers
- CSWE Accreditation
- DSW vs. PhD in Social Work
- Environmental Social Work
- Free Implicit Bias Tests & Training Resources
- How Long Does It Take to Become a Social Worker?
- How Social Work Reduces Healthcare Costs
- How to Find a Social Work Job
- Levels of Social Work Licensure
- LGBTQIAP in Social Work
- Mental Health & Homelessness
- Micro, Mezzo & Macro Social Work
- MSW Admission Requirements
- MSW Scholarships
- MSW Specializations
- MSW vs. MSSW
- Remote Resources for Mental Health Workers
- Social Work & Food Insecurity
- Social Work & Gun Violence Prevention
- Social Work Ethics
- Social Work Field Placement Guide
- Social Work Grants
- Social Work Internships
- Social Work Theories & Practice Models
- Social Work Volunteer Opportunities
- Social Work vs. Counseling
- Social Work vs. Psychology
- Social Work vs. Sociology
- Social Worker Salary Guide
- Social Worker vs. Therapist
- Social Worker's Guide to Cyberbullying
- Student Mental Health & Social Work on College Campuses
- What Can You Do With an MSW Degree? Careers & Salaries
- Why Is Research Important in Social Work? A Complete Guide
- Women in Social Work Leadership