Points of interest…
- LCSWs can diagnose, provide psychotherapy, and bill insurance independently.
- BLS projects 19% job growth for substance abuse counselors through 2033.
- Burnout affects 93% of behavioral health workers, making self-care essential.
More than 48 million Americans met criteria for a substance use disorder in 2022, according to SAMHSA, yet the behavioral health workforce has not kept pace with that demand. Detox centers, residential programs, and outpatient clinics are actively competing for licensed clinicians, and mental health and substance abuse social workers are among the most versatile hires available.
Addiction social work is not simply counseling rebranded. A licensed clinical social worker in a detox setting can diagnose co-occurring disorders, provide psychotherapy, coordinate discharge planning, and bill insurance independently. That scope separates the role from most addiction counselor credentials and explains why MSW graduates are increasingly being recruited into treatment settings that once defaulted to psychology or counseling hires.
The field's central tension is credentialing: an MSW alone does not authorize independent clinical practice. Licensure timelines, supervised hour requirements, and state-specific rules create a gap between graduation and full clinical autonomy that every prospective addiction social worker needs to plan around.
What Does an Addiction Social Worker Do?
Addiction social workers are licensed clinicians who help individuals and families affected by substance use disorders move from crisis to long-term recovery. They combine clinical assessment, therapeutic intervention, and case management within hospitals, detox centers, residential programs, and community agencies. Unlike generalist social workers, these professionals specialize in the physical, psychological, and social dimensions of addiction, often stepping in during the most acute phases of withdrawal and stabilization.
Core Responsibilities in Addiction Settings
A typical day may include conducting biopsychosocial assessments to understand a client's substance use history, mental health status, and social supports. From there, the substance abuse social worker develops a treatment plan that coordinates medical detox, therapy, and aftercare. Crisis intervention is frequent: de-escalating a client in severe withdrawal, responding to suicidal ideation, or managing a relapse. Discharge planning begins almost immediately, linking clients to outpatient therapy, sober living, or 12-step programs. Throughout, the social worker communicates with physicians, nurses, psychiatrists, and peer recovery specialists to ensure continuity of care.
Who Addiction Social Workers Serve
Caseloads span adults and adolescents, families torn apart by addiction, justice-involved individuals, and people with co-occurring mental health disorders. This breadth sets the role apart from general clinical social work, which may focus on a narrower population. An addiction social worker might spend the morning with a young adult overcoming opioid dependence, then run a family session to rebuild trust, and end the day collaborating with probation officers on a client's court-ordered treatment plan.
A Day in the Life: Daniela Sauceda at The Haven Detox Florida
Daniela Sauceda, a 2026 MSW graduate from Florida Atlantic University, now serves as a clinical intern and therapist at The Haven Detox Florida, an inpatient detoxification and rehabilitation facility.1 She applies unconditional positive regard and intentional rapport-building to meet clients where they are, often in the raw, vulnerable first days of sobriety. "Meeting someone in early recovery means showing up without judgment," she explains. "The therapeutic relationship itself becomes the foundation for change." Sauceda's training in trauma-informed care and strengths-based approaches in social work, rooted in her FAU coursework, equips her to see the whole person beyond the addiction.1 Her work mirrors the daily reality of thousands of addiction social workers: walking alongside clients through withdrawal, facilitating group therapy, and planting seeds of hope that will grow in later stages of recovery.
From Direct Practice to System-Level Change
Addiction social workers also shape recovery beyond the clinical hour. At a macro level, they design prevention programs, advocate for policy reform, and lead community coalitions against the opioid crisis. Whether sitting bedside in a detox unit or testifying at a state hearing, the role demands both deep empathy and rigorous clinical skill.
Detox Vs. Residential Vs. Outpatient: How the Setting Shapes Your Work
Where you practice in addiction social work changes almost everything about your daily experience. The clinical interventions are similar across settings, but the pace, your role on the team, and the emotional demands shift considerably depending on whether you are working in detox, a residential program, or an outpatient clinic.
Detox: High Stakes, Short Windows
Detox units sit at the acute end of the care continuum. Patients arrive in medical crisis, and the primary concern is physical stabilization. As a social worker in this environment, you are working alongside physicians and nurses who drive clinical decisions, which means your role centers on brief motivational work, rapid psychosocial assessment, and triage to the next level of care. The emotional load comes in short, intense bursts. Patients cycle through quickly, and forming a therapeutic relationship within 48 to 72 hours requires a particular kind of focus. Per detoxification guidelines from NCBI, the medical risk in this phase is significant, making strong interdisciplinary communication a core competency.1
Residential: Sustained Engagement and Deeper Work
Residential programs offer something detox rarely can: time. Patients stay for weeks or months, which allows for structured group programming, individual therapy, milieu management, and thorough aftercare planning. The team is broader and runs around the clock, often including peer support specialists, case managers, and residential staff alongside clinical professionals. Research on residential rehabilitation indicates that this treatment level generally shows higher completion rates than outpatient options, though the post-discharge period carries its own mortality risks that make careful transition planning essential.2 This setting suits social workers who want depth over breadth in their clinical relationships.
Outpatient: Flexibility and the Challenge of Retention
Outpatient settings serve clients who are managing recovery alongside work, school, and family. Sessions are scheduled rather than continuous, and your coordination role expands to include employers, schools, and community supports. The acuity is lower on average, but outpatient programs face real dropout challenges. Completion rates in outpatient settings tend to lag behind residential programs,3 meaning a large part of your clinical work involves managing engagement and addressing daily life stressors that compete with treatment goals. The intensity of this work, spread across a longer timeline, carries its own sustainability demands, and understanding social worker burnout causes and consequences is worthwhile before committing to any setting.
Choosing the right setting is not just a logistical decision. It reflects the kind of social worker you want to be and the level of intensity you can sustain over a career.
Questions to Ask Yourself
MSW Pathways and Addiction Specializations
Most MSW programs offer two concentration tracks that align with addiction practice: clinical social work (sometimes called advanced clinical practice) and health or behavioral health. The clinical track emphasizes direct therapeutic intervention, diagnosis, and individual or group counseling, skills central to detox and recovery settings. The health or behavioral health track often integrates public health frameworks, community-level interventions, and chronic disease management, which can include substance use disorder treatment in hospital or outpatient contexts. Not every program labels its addiction coursework identically. You may see electives or certificate tracks titled substance abuse treatment, addiction counseling, or chemical dependency, all pointing to the same competency set.
Core Coursework That Prepares You for Substance Use Practice
Regardless of track title, five content areas recur across strong addiction-focused MSW curricula:
- Psychopharmacology: Understanding how substances affect brain chemistry, withdrawal timelines, and medication-assisted treatment (methadone, buprenorphine, naltrexone) so you can collaborate with prescribers and educate clients.
- Co-occurring disorders: Learning to assess and treat clients whose substance use intersects with depression, anxiety, PTSD, or severe mental illness, conditions present in the majority of detox admissions.
- Group therapy: Developing facilitation skills for process groups, psychoeducational sessions, and relapse-prevention workshops, the backbone of residential and outpatient programming.
- Motivational interviewing: Mastering the reflective listening and change-talk techniques that move ambivalent clients toward readiness, especially critical in early detox and pre-contemplation stages.
- Trauma-informed care: Recognizing the prevalence of adverse childhood experiences and trauma histories among people with addiction, and adapting interventions to avoid retraumatization.
Programs that embed these topics across multiple courses, rather than isolating them in a single elective, produce graduates who can integrate social work theories and practice models from day one.
Field Placement: The Single Biggest Differentiator
Your practicum site matters more than your transcript. A placement at a detox facility, methadone clinic, residential treatment center, or recovery housing program gives you supervised client contact, documentation experience under state standards, and professional references in the addiction field. Employers hiring for substance use positions consistently prioritize candidates who completed relevant internships over those with generic hospital or child welfare placements. If you are still weighing programs, MSW field placement tips can help you evaluate how well a program supports placement in addiction settings.
Daniela Sauceda's trajectory illustrates this principle. After earning a bachelor's degree in psychology, she entered Florida Atlantic University's MSW program and secured a clinical internship at The Haven Detox Florida.1 That placement allowed her to apply unconditional positive regard and rapport-building techniques in real time, working alongside licensed clinicians during acute withdrawal and stabilization. By graduation in 2026, she had both the credential and the demonstrable competence to continue as a therapist at the same facility, an outcome that traces directly to intentional placement selection during her program.
Related Articles
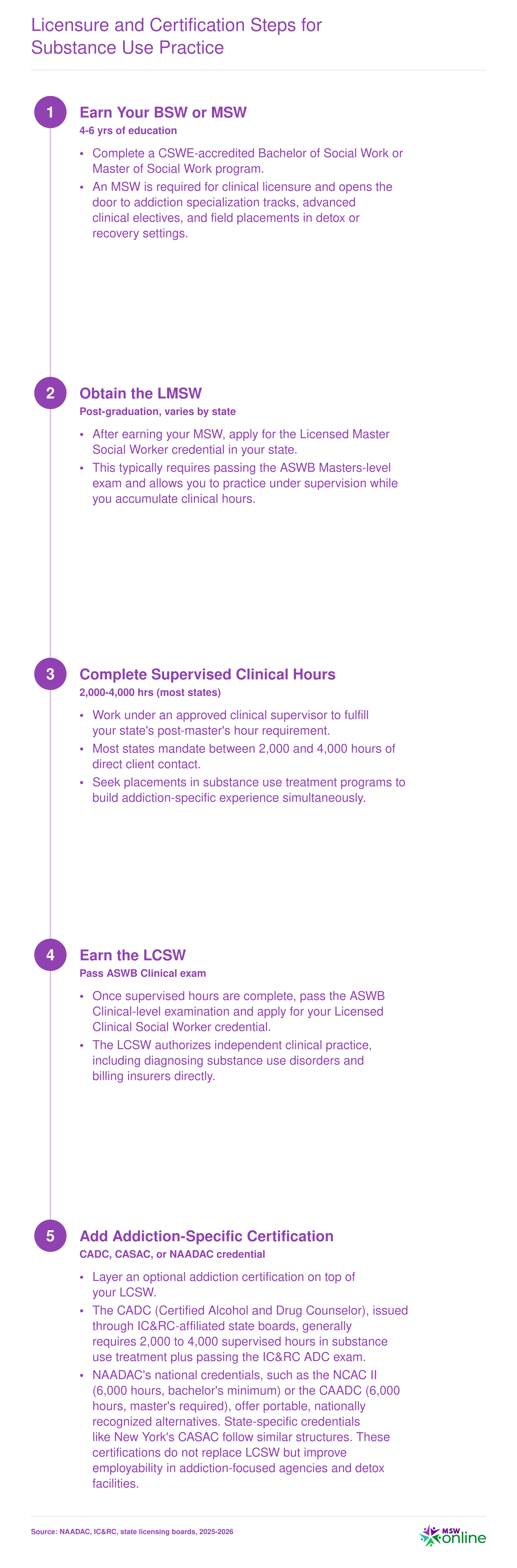
Licensure and Certification Steps for Substance Use Practice
Practicing clinical social work in addiction settings requires a layered credentialing process. You will first earn your social work license, then add optional addiction-specific certifications that signal specialized expertise. Requirements vary by state, so confirm your jurisdiction's exact hour thresholds, approved supervisors, and exam formats before you begin accruing post-master's hours.
Social Worker Vs. Addiction Counselor: Key Differences
Employers in detox facilities, outpatient clinics, and residential programs increasingly post openings for both licensed clinical social workers and certified addiction counselors, often side by side on the same treatment team. Understanding the credentials, scope, and trajectory of each role helps you choose the path that aligns with your education, budget, and long-term goals.
Education and Credential Pathways
Licensed clinical social workers hold a Master of Social Work degree, complete two years of supervised clinical hours (typically 3,000), and pass a national exam to earn the LCSW credential. The MSW curriculum covers human behavior, policy, research, and a range of clinical theories, with electives or concentrations in addiction available at many programs.
Certified addiction counselors enter the field with education ranging from a high school diploma to a bachelor's degree. Programs like the Certified Alcohol and Drug Counselor (CADC) or Certified Alcoholism and Substance Abuse Counselor (CASAC) require targeted coursework in substance use disorder counseling, supervised hours specific to addiction treatment (often 1,000 to 6,000 hours depending on the state), and a certification exam.2 Many counselors enter the field with lived experience or peer backgrounds and pursue formal certification afterward.
Scope of Practice and Clinical Autonomy
For a closer look at how these roles compare in practice, the social work versus counseling degrees and licensure breakdown covers key distinctions worth reviewing. LCSWs carry a broad scope: they can diagnose mental health and substance use disorders, deliver psychotherapy for co-occurring conditions, provide case management, engage family systems, and bill insurance directly.3 This breadth allows clinical social workers to address the full spectrum of biopsychosocial factors driving addiction.
Addiction counselors focus on substance use education, group facilitation, relapse prevention, and motivational interviewing. Their scope is narrower and varies by state; in many jurisdictions, they must work under the supervision of a licensed clinician and cannot independently diagnose or practice psychotherapy outside the SUD domain.3 Some states grant advanced counselor credentials (LADC, LCADC) that expand autonomy, but these often require additional hours and clinical training.2
Salary and Career Trajectory
Salary data reflects the education and scope differences. LCSWs in substance abuse roles typically earn median salaries in the mid-50,000 to low-70,000 dollar range, with private practice and supervisory positions pushing into six figures. Certified addiction counselors earn median salaries in the low-to-mid 40,000 dollar range, with more limited upward mobility unless they pursue graduate-level licensure.
Career paths also diverge. MSW versus LCSW degree and license differences are worth understanding early, because LCSWs can transition into clinical supervision, program administration, policy advocacy, research, and private practice. Addiction counselors primarily advance within SUD programs, moving from direct counseling to team lead or coordinator roles. Higher administrative or clinical director positions in most agencies require a master's degree and independent licensure.4
Scope of practice is the dividing line. An LCSW can diagnose mental health and substance use disorders, provide psychotherapy, and bill insurance independently. Most addiction counselors cannot do any of those things without supervision. That difference is why LCSWs command higher salaries and reach clinical director roles that stay closed to counselor-only credentials.
Addiction Social Worker Salary and Job Outlook
The table below draws on 2024 wage estimates from the Bureau of Labor Statistics Occupational Employment and Wage Statistics survey. Because the BLS does not break out a standalone category for addiction social workers, the figures reflect broader occupation groups that include substance use roles alongside mental health and other specializations. Addiction social workers who hold clinical licensure (such as the LCSW), work in metropolitan hospital or detox settings, or carry additional certifications like the CADC typically earn toward the 75th percentile or above within their occupation category.
| Occupation | Total Employment (2024) | 25th Percentile Salary | Median Salary | 75th Percentile Salary | Projected Job Growth |
|---|---|---|---|---|---|
| Substance Abuse, Behavioral Disorder, and Mental Health Counselors | 440,380 | $47,170 | $59,190 | $76,230 | 18.4% (2022 to 2032) |
| Social Workers (All) | 759,740 | $48,680 | $61,330 | $78,500 | 6% (2024 to 2034) |
| Child, Family, and School Social Workers | 382,960 | $47,480 | $58,570 | $74,060 | N/A |
| Healthcare Social Workers | 185,940 | $55,360 | $68,090 | $83,410 | N/A |
| Counselors, Social Workers, and Community/Social Service Specialists (All) | 2,477,920 | $45,750 | $57,480 | $75,090 | N/A |
Highest-Paying States for Substance Abuse Social Workers
The table below ranks the top-paying states for substance abuse, behavioral disorder, and mental health counselors by median annual salary, based on 2024 data from the Bureau of Labor Statistics. States with the highest pay often reflect a combination of elevated cost of living, robust treatment infrastructure, and strong demand for qualified professionals. Keep in mind that a higher median salary does not always translate to greater purchasing power once housing and living expenses are factored in.
| State | Median Annual Salary | Mean Annual Salary | Total Employment |
|---|---|---|---|
| Alaska | $79,220 | $88,870 | 1,060 |
| New Mexico | $70,770 | $71,010 | 2,070 |
| Oregon | $69,660 | $72,860 | 6,410 |
| North Dakota | $66,450 | $68,220 | 1,180 |
| District of Columbia | $66,140 | $71,200 | 980 |
| Utah | $65,920 | $71,890 | 4,720 |
| Idaho | $65,240 | $65,290 | 2,130 |
| New Jersey | $64,710 | $75,900 | 14,640 |
| Nebraska | $64,410 | $66,690 | 1,980 |
| Washington | $64,220 | $70,230 | 13,150 |
| Arizona | $63,830 | $67,890 | 8,970 |
| Connecticut | $62,960 | $66,920 | 6,470 |
| Wisconsin | $62,470 | $70,180 | 9,450 |
| New York | $62,070 | $69,290 | 22,450 |
| Wyoming | $61,640 | $65,650 | 840 |
Essential Skills, Interventions, and Clinical Competencies
Essential skills for addiction social work aren't abstract theories; they are practical, evidence-based tools that you use every day to engage clients, reduce harm, and support recovery. The most effective social workers in detox and recovery settings build a clinical toolkit around four core competencies: motivational interviewing, harm reduction, trauma-informed care, and collaboration with medication-assisted treatment prescribers.
Motivational Interviewing: The Cornerstone of Addiction Practice
Motivational interviewing (MI) is more than a technique; it's the foundational communication style that aligns with social workers' ethical responsibilities to clients, particularly the commitment to client self-determination. MI helps you meet individuals wherever they are in the stages of change, using reflective listening and open-ended questions to explore ambivalence about substance use without confrontation. Because addiction often involves cycles of relapse and recovery, MI strengthens the therapeutic alliance and empowers clients to voice their own reasons for change. It's a skill that directly translates into better engagement in detox and outpatient settings.
Harm Reduction and Trauma-Informed Care
Two overlapping frameworks define modern addiction social work. Harm reduction meets clients with practical strategies to reduce negative consequences, think safer use, managed use, or medication-assisted pathways, rather than demanding immediate abstinence. It pairs naturally with trauma-informed care (TIC), which recognizes that many individuals with substance use disorders have histories of trauma. TIC shifts the question from "What's wrong with you?" to "What happened to you?" and guides you to create physical and emotional safety in every interaction. Together, these frameworks let you address immediate risks while building trust for deeper therapeutic work.
A related competency that employers increasingly expect is the ability to assess co-occurring disorders. Most individuals in addiction treatment have concurrent mental health conditions such as PTSD, depression, or anxiety. Knowing how to screen for these, understand their interplay with substance use, and refer for integrated care is no longer optional; it's core to effective clinical social work.
Collaborating with Medication-Assisted Treatment Prescribers
Medication-assisted treatment (MAT) uses FDA-approved medications like buprenorphine, methadone, or naltrexone alongside counseling. As a social worker, you may not prescribe these medications, but you play a critical role in coordinating with prescribers, monitoring side effects, and helping clients adhere to their treatment plan. Understanding the science behind MAT reduces stigma and lets you advocate for clients who face judgment from peers or family members. This interdisciplinary collaboration is a non-negotiable skill in detox, residential, and outpatient programs.
Soft Skills that Set You Apart
Clinical knowledge gets you in the door; these interpersonal abilities keep you effective: - Boundary-setting: You'll build deep relationships with clients, but clear professional boundaries protect both you and them from burnout or ethical drift. - Cultural humility: Addiction does not discriminate, and every client brings a unique cultural context. Staying curious and open without making assumptions is essential. - Tolerance for ambiguity: Recovery rarely follows a straight line. You need comfort with uncertainty, knowing that a lapse today doesn't erase progress and that some clients will re-enter treatment multiple times before reaching stability.
Burnout, Self-Care, and Sustaining a Long Career in Addiction Treatment
Addiction treatment is quietly hemorrhaging its workforce, and the field is finally treating that as a systems problem rather than a personal failing. A 2023 National Council for Mental Wellbeing survey found that 93% of behavioral health workers reported experiencing burnout, with 62% reporting moderate to severe burnout and nearly half (48%) considering leaving their jobs.1 A 2024 NIH review of social workers specifically found elevated emotional exhaustion in 73% of clinicians and high depersonalization in 26%, both of which correlate directly with turnover and reduced client outcomes.2
What Drives Burnout in Substance Use Settings
Addiction social work carries stressors that generalist practice does not. Relapse is part of the recovery process, but repeated cycles wear on clinicians who measure progress in months of sobriety. Involuntary discharge policies, common in detox and residential settings, produce moral distress when a clinician must terminate care with someone still in acute risk. Vicarious trauma accumulates from client histories involving overdose, abuse, and loss. Layered on top: chronic underfunding, high caseloads, and a projected shortage of roughly 31,000 mental health practitioner FTEs by 2025,1 even as demand for substance use social workers is projected to grow 14% while supply contracts by 2%.3 MSW clinical year burnout is one early warning sign students often encounter before they fully grasp how those structural pressures compound over a career.
Evidence-Based Strategies That Actually Work
- Clinical (not administrative) supervision: Regular reflective supervision focused on countertransference, moral distress, and case formulation, distinct from productivity check-ins.
- Reflective practice groups: Peer consultation groups where clinicians process difficult cases and normalize vicarious trauma responses.
- Workload boundaries: Documented caseload caps, protected non-clinical time, and no-contact windows outside scheduled hours.
- Organizational interventions: Trauma-informed leadership, transparent staffing ratios, and paid time for continuing education and debriefing after critical incidents such as client deaths.
Sustainability Is a Structural Issue
NASW guidance is explicit that employers, not individual clinicians, hold primary responsibility for workplace conditions that prevent burnout. That includes reasonable caseloads, access to clinical supervision, mental health benefits, and cultures that treat leave-taking as legitimate rather than a sign of weakness. Prospective addiction social workers should evaluate employers on these terms during interviews. Ask about caseload numbers, supervision structure, and turnover rates. A program that cannot answer those questions clearly is telling you something important about how long its clinicians tend to stay.
From Entry-Level to Director: The Addiction Social Work Career Ladder
Addiction social work offers a clear progression from supervised trainee to organizational leader, with each stage unlocking greater clinical autonomy and earning potential. The ladder typically spans 10 to 15 years for clinicians who pursue licensure and supervisory credentials on a standard timeline. A parallel macro-practice track leads to policy and systems-level roles at agencies such as state substance use authorities or SAMHSA.
Frequently Asked Questions About Addiction Social Work
Below are answers to some of the most common questions prospective and practicing social workers ask about building a career in addiction treatment. For deeper explanations, refer to the relevant sections earlier in this guide.