Points of interest…
- Pittsburgh's June 2026 co-response pairs one officer with one clinician in all seven police zones plus Downtown.
- Program goals are reducing arrests, ER visits, and increasing access to treatment for mental health crises.
- Co-response clinicians need an MSW, licensure, and crisis intervention training; funding blends Medicaid with federal grants.
- Integrated teams have cut arrests and emergency room use nationally, but dual loyalty dilemmas persist for social workers.
Under Pittsburgh's previous model, social workers responded to mental health crises separately from police. On June 17, 2026, the city replaced that siloed approach with a co-response team embedding one officer and one clinician per police zone. That structural shift mirrors a national pattern: cities are moving from fragmented crisis response toward integrated units where social workers and law enforcement operate as a single resource. For MSW-trained clinicians, the expansion turns crisis intervention into a mainstream career path, as Denver, Dallas, and now Pittsburgh are funding permanent positions, not temporary pilots.
Clinicians stepping into these roles face dual loyalties, scene safety demands, and ethical complexities that graduate programs rarely simulate. The speed of adoption presses the profession to develop clearer training standards and practice guidelines for police-embedded social work.
Pittsburgh's Co-Response Team: What Changed in 2026
Pittsburgh's renewed co-response program embeds a mental health clinician directly with a police officer, sending them to crisis calls as a single unit rather than separate responders. Announced on June 17, 2026, the model reflects a deliberate shift away from earlier approaches that sent social workers independently to scenes.
From Separate Response to Embedded Partnership
Under former Mayor Gainey, social workers responded separately from police, often arriving after officers had already contained a situation. The current administration prioritized joint deployment. Public Safety Director Sheldon Williams explained, "This is a supplement to that level of response" , meaning the clinician works alongside the officer, not as his or her replacement. Mayor Corey O'Connor underscored the practical rationale: "Not every call needs someone in uniform to show up," yet the partnership ensures that appropriate support is immediately available.
Staffing and Dispatch Structure
The program assigns one Pittsburgh Police officer and one mental health clinician to each of the city's seven police zones, with an additional team dedicated to Downtown due to higher call volume. All teams operate from police headquarters, which streamlines dispatch and fosters real-time collaboration. Lieutenant Anthony Cunningham, the program's executive officer, and Sergeant Colleen Bristow provide ongoing leadership and evaluation. The structure means that clinicians are fully integrated into day-to-day operations rather than being on call from an outside agency.
Stated Goals and Evaluation
Police Chief Jason Lando framed the relaunch as more than a simple return: "Today's announcement is not just about bringing back a program. It's about building a stronger and better version of it." The articulated goals are concrete: reduce unnecessary arrests, decrease emergency room visits, and increase access to mental health treatment. Chief Lando noted that officers respond to mental health calls daily, making consistent clinician presence a practical necessity. The evaluation framework under Cunningham and Bristow will track these outcomes, offering data that may influence future scaling.
A Growing Niche for MSW Graduates
For social work professionals, Pittsburgh's model signals a career path in which MSW graduates hold salaried, clinical positions embedded within law enforcement. These roles demand specialized crisis intervention skills and social worker safety in mental health settings, along with interagency collaboration competencies that many Master of Social Work programs are now building into curricula. As more municipalities explore co-response, the demand for licensed clinicians comfortable working alongside police is likely to increase, creating stable, direct-service jobs for new graduates.
How Does a Co-Response Team Work?
Across the country, 911 centers are increasingly embedding behavioral health expertise into dispatch decisions, transforming law enforcement's default response to mental health crises. Underneath that shift lies a deliberate operational wiring that routes the right kind of help to the right calls.
From 911 Call to Co-Response Deployment
The pathway starts when a 911 dispatcher or embedded clinician applies structured screening questions about weapons, threats, self-harm, and medical needs.1 Call-takers in many jurisdictions now have direct access to behavioral health specialists who provide real-time input, turning the dispatch center into a sorting point rather than a one-size-fits-all response engine. Co-response teams are dispatched when the primary issue appears to be behavioral health but some level of safety risk remains, enough that sending a civilian-only team would be unwise, but not so severe that a full law enforcement response is required.2 Standard police patrols still answer calls involving credible threats of violence, active weapons, or immediate public safety dangers, while civilian mobile crisis teams, often reachable through 988 or specialty crisis lines, handle situations with no weapons and low risk of harm.1 In Durham's HEART program, for instance, 911 call-takers route calls to four distinct units: Crisis Call Diversion, Community Response Teams, Co-Response, or an Involuntary Commitment Response Team, all based on real-time triage, with residents always dialing 911 as the single entry point.3
On-Scene Coordination: Officer and Clinician Roles
Once a co-response team arrives, role boundaries are clear and complementary. The police officer manages scene safety, physical threat assessment, and any legal authority needed, while the mental health clinician takes the lead on behavioral assessment, de-escalation, and connection to care.2 They communicate constantly, with the clinician often making first verbal contact to gauge the individual's state and reduce tension. If the situation escalates, the officer can intervene; if it stabilizes, the clinician continues the clinical conversation. This real-time coordination avoids the fragmented handoffs that occur when police and social workers operate in separate timelines, as Pittsburgh's earlier model under former mayor Ed Gainey demonstrated.
Handoffs and Continuity of Care
A co-response encounter does not end when the team leaves. The clinician proactively makes warm referrals, direct and scheduled linkages to outpatient treatment, medication management, or peer support, and often coordinates with county mobile crisis teams and the 988 Suicide & Crisis Lifeline network to ensure no gap in care.1 Fairfax County's co-responder program aligns its workflow with Virginia's Marcus Alert law, which requires 911, crisis call centers, and behavioral health agencies to share patient information and follow-up responsibilities.4 Protocols typically include a defined follow-up window during which the clinician checks on the individual's engagement and adjusts the care plan as needed.
How Co-Response Differs from Other Crisis Models
It is easy to conflate co-response with standalone civilian crisis teams or CIT-only policing. Standalone mobile crisis units, like Denver's STAR van dispatched by 911 or Tucson's MCRT accessed through crisis lines integrated with 988, send unarmed clinicians and peer specialists to low-risk, non-violent behavioral health calls with no officer present on scene.5 CIT-only models train officers extensively in de-escalation and mental health awareness but leave them to navigate crisis encounters alone, without an embedded clinician to take over the therapeutic work. Co-response deliberately pairs the two skill sets, giving communities a middle path that retains the safety net of sworn personnel while empowering social workers to redirect people away from arrests and emergency rooms, a balance that cities like Pittsburgh, Durham, and Fairfax County are betting on for calls that fall in the gray zone between clear danger and clear safety.
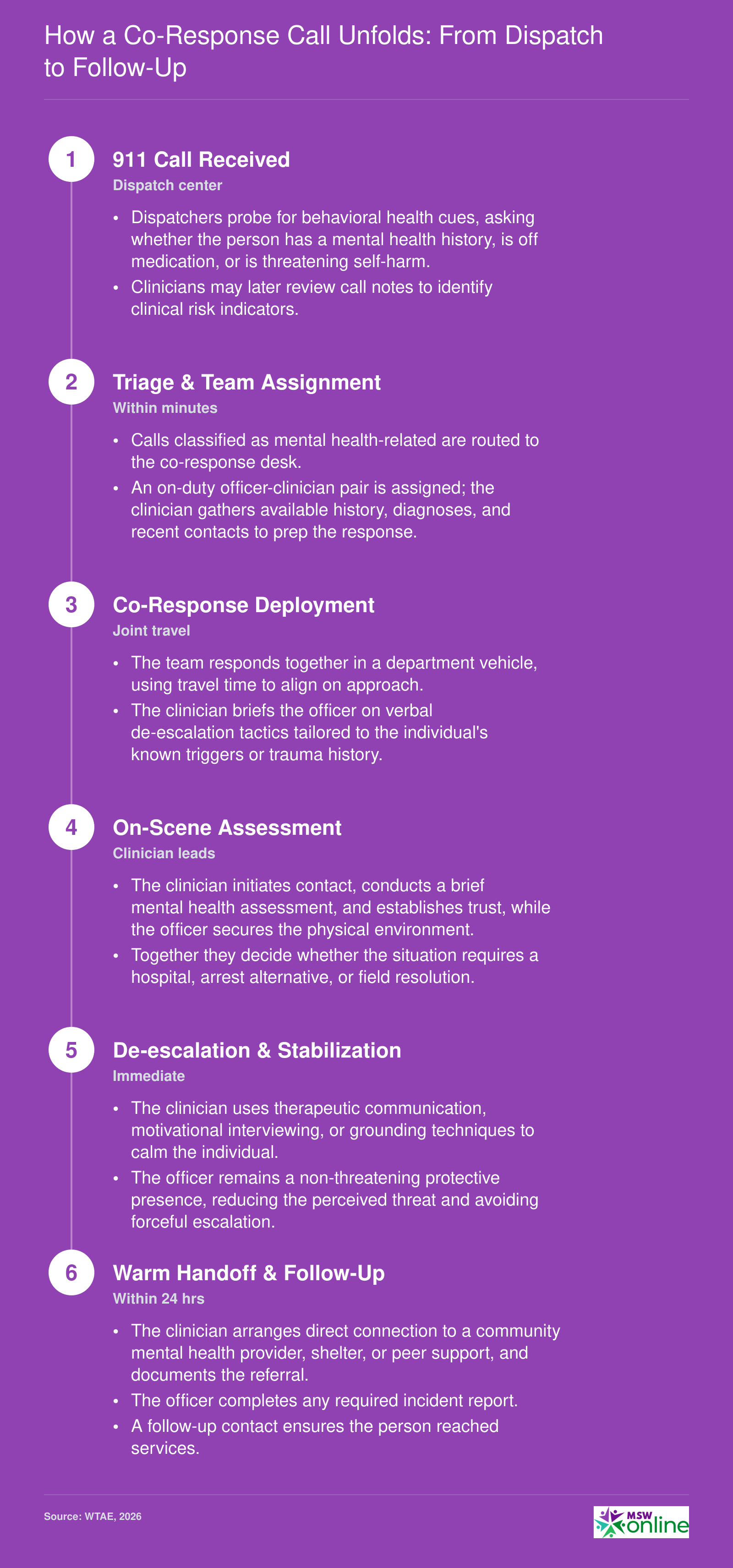
How a Co-Response Call Unfolds: From Dispatch to Follow-Up
Pittsburgh's 2026 co-response teams follow a structured workflow designed to bring behavioral health expertise to the front end of a crisis. At each stage, the clinician and officer work together to de-escalate, assess, and connect individuals to services rather than defaulting to arrest or emergency room transport.
Co-Response Vs. Other Crisis Models in Pennsylvania
Pennsylvania communities are adopting varied approaches to mental health crisis response, moving beyond the traditional law-enforcement-only model. Understanding the differences among these models is essential for social workers evaluating career paths and for agencies designing effective interventions. The primary models fall into three categories: embedded co-response, where a clinician rides with an officer; sequential co-response, where a clinician is called after police secure the scene; and community-based mobile crisis, which excludes police unless necessary for safety.
Pittsburgh's Embedded Co-Response Model
Pittsburgh's 2026 relaunch places a police officer and a mental health clinician together in a single unit, dispatched simultaneously from police headquarters. This embedded structure lets the clinician assess immediately alongside law enforcement, aiming to de-escalate, connect individuals to care, and reduce unnecessary arrests or emergency room visits. The team covers all seven police zones, with an extra unit downtown due to higher call volume.
Other Pennsylvania Approaches
A scan of active programs outside Pittsburgh reveals a spectrum of designs:
- Bucks County: Sequential co-response model. Masters-level social workers operate as mobile co-responders. Police arrive first, then call the clinician once the scene is secure. Seven co-responders serve the county.1
- Dauphin County: Hybrid co-responder and mobile crisis team. Ten behavioral health clinicians are dispatched with or immediately after police, allowing flexibility based on call risk.2
- Elizabethtown Borough: Peer recovery co-responder program. Certified Peer/Recovery Specialists respond together with police officers to selected emergency calls, focusing on substance use and behavioral health.3
- West Lampeter Township: Similar peer recovery model. Certified Recovery Specialists ride with officers to calls involving substance use, bridging law enforcement and community treatment.4
Key Differentiators Across Pennsylvania
- Staffing: Pittsburgh and Bucks County deploy master's-level or licensed clinicians, while several smaller municipalities use certified peer specialists. The clinician model emphasizes diagnostic ability and therapeutic intervention; the peer model prioritizes shared lived experience.
- Dispatch method: Embedded teams like Pittsburgh's dispatch the clinician simultaneously with the officer. Sequential models wait for police to clear the scene. Peer programs often integrate with officers from the outset but may focus on nonviolent, substance-related calls.
- Hours and availability: Hours vary widely. Some programs operate during business hours only, while others, like Pittsburgh's, work toward 24/7 rotations. Coverage often depends on staffing size and call demand.
- Funding sources: Programs are sustained through a mix of county mental health allocations, state grants, federal SAMHSA dollars, and local police budgets. Sustainability remains a challenge for pilot initiatives lacking permanent funding streams.
These models demonstrate how social workers can practice outside traditional clinical offices, taking on crisis intervention roles that directly intersect with public safety. For MSW programs in Pennsylvania, familiarity with co-response structures and their operational nuances can open doors to specialized positions in law enforcement agencies, county crisis systems, and peer-run organizations.
Mayor O'Connor said, "Not every call needs someone in uniform to show up," positioning co-response as a precision tool, not a substitute for policing. This distinction is vital for social workers: integrated teams apply clinical skills to mental health calls, complementing law enforcement's role.
Program Goals and Outcome Metrics
Pittsburgh's co-response relaunch is explicitly built around measurable outcomes that determine whether the model actually diverts individuals from arrest, emergency rooms, and repeat crises.
Pittsburgh's Stated Goals and Evaluation Structure
The city has defined three core aims: reduce unnecessary arrests, decrease emergency department visits, and increase access to behavioral health treatment. Police Chief Jason Lando reinforced this focus by stating, "Today's announcement is not just about bringing back a program. It's about building a stronger and better version of it." That stronger version includes a formal evaluation structure led by Lt. Anthony Cunningham and Sgt. Colleen Bristow, who are responsible for tracking call dispositions, service linkages, and diversion rates across all seven police zones, with heightened attention to the higher-volume Downtown area. Their work is designed to replace anecdotal impressions with concrete data that can inform future staffing, training, and budget decisions.
National Co-Response Benchmarks
Pittsburgh's framework draws on a growing body of evidence from other jurisdictions. In Colorado, co-responder teams handled more than 25,900 calls during a single two-year period (2020-2021) and achieved a 98% arrest avoidance rate, with only 2% of encounters resulting in arrest.1 Fully 86% of individuals were connected directly to community-based services.1 In Burlington, North Carolina, a co-responder program evaluation found a 28-30% relative reduction in emergency room transports compared to police-only responses, dropping from a 26.2% transport rate to 18.75%.2 National reviews of high-utilizer interventions report 50-70% reductions in crisis-related hospitalizations.3 Financially, the Texas PICC program alone saved an estimated $3 million in ER costs in 2021, while broader analyses estimate that a single co-responder team can yield roughly $350,000 in annual cost savings through diverted arrests and hospitalizations.4 Programs like Johnson County's in Kansas have also documented meaningful reductions in repeat calls, signaling that the benefits compound when individuals are connected to ongoing care.5
Pennsylvania's Data Gap and the Value of Standardized Metrics
Despite these national benchmarks, Pennsylvania-specific outcome data remains thin. The Pittsburgh relaunch essentially begins a new data collection cycle, and few peer programs in the state have published rigorous evaluations. This gap matters because standardized metrics are the currency of program sustainability: without shared definitions of "diversion" or "linkage to care," it is difficult for municipalities to compare models, secure state or federal funding, or build legislative support for expansion. Groups like the SAMHSA GAINS Center and the Police Executive Research Forum have urged jurisdictions to adopt common indicators including arrest rates, ER utilization, repeat contact, and cost per encounter, precisely so that co-response can move from pilot to permanent fixture.
Outcome Tracking as a Social Work Competency
For MSW-educated clinicians working inside these teams, understanding importance of research in social work is not an administrative afterthought but a professional obligation. The NASW Code of Ethics calls on social workers to monitor and evaluate policies, programs, and practice interventions. In co-response settings, that means pushing beyond crisis de-escalation to document whether a person was connected to a mental health clinic, prescribed medication, or shown a path to housing. Social workers who can collect and interpret these outcome data elevate their own role from first responder to systemic change agent, making the case for why co-response belongs in every police department's toolkit.
Co-Response Outcomes at a Glance
National evaluations of co-response programs consistently report fewer arrests, lower emergency department usage, and significant cost savings when mental health clinicians ride alongside law enforcement.

Related Articles
Training Requirements for Police Social Workers
What credentials and training do you need to work as a social worker on a police co-response team?
Baseline Credentials: MSW and State Licensure
To function as a co-response clinician, a Master of Social Work (MSW) from a Council on Social Work Education (CSWE)-accredited program is almost always required. In Pennsylvania, the state licensure board mandates that clinical social work roles hold either a Licensed Social Worker (LSW) credential, which requires passing the ASWB Master's exam, or a Licensed Clinical Social Worker (LCSW) designation, which adds 3,000 hours of supervised post-master's experience and a clinical exam. Most police departments and mental health agencies prefer or require the LCSW because it allows independent diagnostic and treatment authority. While some programs may employ BSW-level staff in support roles, the direct co-response clinician role is firmly a master's-level position due to the need for autonomous clinical judgment during field crises.
Specialized Crisis Intervention Training
Earning an MSW and license is just the starting point. Co-response social workers complete specialized training that often overlaps with law enforcement curricula. The most common model is Crisis Intervention Team (CIT) training, a 40-hour program that teaches officers and mental health professionals to recognize psychiatric symptoms, de-escalate volatile situations, and connect individuals to appropriate services. Social workers also receive instruction in trauma-informed care certifications to avoid re-traumatizing individuals during police encounters, and they practice suicide risk assessment using structured tools like the Columbia-Suicide Severity Rating Scale (C-SSRS). Joint de-escalation exercises with officers build trust and shared language, ensuring both partners can manage a scene safely while prioritizing the individual's mental health needs over punitive actions.
Supervision and Accountability Structures
A unique challenge for police social workers is navigating dual accountability. Clinically, they are supervised by a licensed clinical supervisor (often an LCSW within a mental health agency or the police department's behavioral health unit) who ensures adherence to social work ethics, scope of practice, and quality of care. Operationally, they report to a police chain of command for deployment, safety protocols, and interagency coordination. This dual structure preserves the social worker's clinical independence while embedding them in law enforcement's rapid-response environment. Continuing education is mandatory to maintain licensure; Pennsylvania requires 30 hours of CE credits every two years, with specific ethics and suicide prevention topics. Many co-response clinicians also pursue advanced certifications in forensic social work or crisis intervention.
The National Training Gap and Pittsburgh's Approach
Currently, no universal national standard exists for police social worker training. Curriculum and credentialing vary widely by jurisdiction, with some programs relying on in-house mentorship and others adopting piecemeal external courses. This gap can lead to inconsistent service quality. Pittsburgh's 2026 relaunch intentionally addresses this by building its own structured training program for the revamped co-response teams. According to police and city officials, the training is being designed to align with the program's goals of reducing arrests, decreasing emergency department visits, and increasing treatment access. This localized approach represents both an opportunity, tailoring content to Pittsburgh's call volume and demographic needs, and a limitation, as it lacks a portable national certification that social workers could carry across agencies. For MSW graduates and experienced clinicians, pursuing a career in this field means staying informed about evolving training models and advocating for evidence-based, standardized practices.
Questions to Ask Yourself
Funding and Sustainability of Co-Responder Programs
Funding a co-response team means securing the financial resources to pay for mental health clinicians, training, equipment, and ongoing program operations. With the right mix of federal, state, and local support, programs can move from pilot phases to permanent crisis response fixtures.
Federal Grants Supporting Co-Response
In 2026, several federal grant programs can directly or indirectly fund co-responder initiatives. The Substance Abuse and Mental Health Services Administration (SAMHSA) distributes block grants to states; Pennsylvania received over $15 million this year.1 While block grants offer flexibility, targeted programs like Project AWARE ($56.17 million across 37 awards) and Certified Community Behavioral Health Clinic (CCBHC) grants ($94 million for planning/development and another $94 million for improvement/advancement) provide dedicated mental health funding.2 These grants have spring deadlines, so planning ahead is essential. - CCBHC Improvement and Advancement Grant: applications closed March 31, 2026.2 - Project AWARE: applications closed April 1, 2026.2 - CCBHC Planning, Development & Implementation Grant: applications closed May 1, 2026.2 - National Child Traumatic Stress Initiative Category III: applications closed May 1, 2026.2
Additional relevant programs include the Assisted Outpatient Treatment Grant Program ($10 million) and the Children's Mental Health Initiative ($43 million). The Implementing Zero Suicide in Health Systems grant ($16.1 million) can also support crisis system infrastructure.3
State and Local Funding in Pennsylvania
Pennsylvania agencies offer complementary funding streams. The Department of Human Services administers block grants and is exploring Medicaid billing provisions for crisis services, which can provide sustainable reimbursement. The Office of Attorney General runs local law enforcement grants that sometimes support mental health partnerships. Monitoring these agencies' websites is critical because state funding cycles may differ from federal ones and can respond to local legislative priorities.
Finding and Applying for Grants
Start with the SAMHSA GAINS Center, which provides technical assistance and maintains up-to-date listings of grant opportunities, application cycles, and awarded projects.4 The COPS Office Community Policing Development grants are another primary source, funding law enforcement initiatives that include mental health collaboration. For practical examples, the National Association of Counties (NACo) and the Council of State Governments (CSG) Justice Center publish case studies of funded co-responder programs, offering insights into successful models and budgeting strategies. Practitioners seeking broader social work grants for practitioners will find additional funding streams applicable to co-response roles. When applying, emphasize data-driven outcomes, interagency partnership letters, and a sustainability plan beyond the grant period. Technical assistance from GAINS can strengthen your proposal.
Ethical and Legal Considerations for Social Workers in Policing
Co-response programs are reshaping the ethical boundaries of clinical social work, but many practitioners find that existing guidelines offer only partial cover for the realities of crisis scenes.
Navigating Dual Loyalty on Scene
- Core tension: The social workers' ethical responsibilities to clients, as defined by the NASW Code of Ethics, prioritize client self-determination and confidentiality, yet co-response embeds social workers in a law enforcement environment where public safety directives can override therapeutic neutrality.
- Practical impact: A clinician may assess that a person needs voluntary treatment, while the officer determines an involuntary hold is necessary based on imminent danger statutes.
- Resolving the conflict: Best-practice programs establish clear protocols that elevate clinical judgment for health decisions and reserve the officer's authority for imminent physical safety threats.
Information-Sharing Under HIPAA and 42 CFR Part 2
- HIPAA boundaries: Clinicians can disclose protected health information to law enforcement only in specific exceptions, such as credible threats of harm or mandatory reporting. Routine operational sharing is not permitted.
- Substance use records: 42 CFR Part 2 adds stricter protections for substance use disorder treatment records, often requiring separate written consent even from other healthcare providers.
- Documentation hygiene: Co-response programs typically maintain separate clinical notes that do not enter police records. Memoranda of understanding (MOUs) often specify that clinical documentation is stored in the behavioral health agency's system, inaccessible to the police department without a valid release or court order.
Informed Consent in Real Time
- On-scene challenge: A person in crisis may not fully understand that the clinician is a mandated reporter, that confidentiality has limits, and that the officer is listening.
- Current practice: Clinicians introduce their role immediately: "I'm a social worker with the crisis team; I'm here to help, and this officer is here to keep everyone safe. What you tell me is confidential unless there's a safety risk." Programs train officers to briefly step back during the clinical assessment whenever possible.
Emerging Protections and Best Practices
- MOUs as guardrails: Formal agreements between police departments and behavioral health agencies define information-sharing limits, supervision structures, and liability lines. Pittsburgh's renewed model embeds clinicians at police headquarters but separates clinical data systems.
- Clinical supervision: Programs assign licensed supervisors without law enforcement ties to regularly review cases for ethical dilemmas, dual-relationship risks, and documentation compliance.
- Separate documentation systems: Evidence shows that when clinical notes stay within a healthcare electronic record and police reports remain in a law enforcement database, both patient privacy and legal defensibility improve.
Public Safety Director Sheldon Williams clarified that co-response is "a supplement to that level of response," not a substitute for police. For social workers, this means embedding mental health expertise within law enforcement rather than supplanting police authority, which sharpens role identity and interprofessional boundaries.
Career Paths: Working as a Social Worker in Law Enforcement
Typical Roles in Police Departments
Social workers inside law enforcement agencies fill several distinct functions. The most visible is the embedded co-response clinician, who rides with officers to mental health crisis calls. Other roles include police department victim advocate, supporting survivors of domestic violence or violent crime; crisis intervention specialist, who trains officers and consults on volatile scenes; and re-entry or diversion coordinators, who connect justice-involved individuals with housing, treatment, and employment to reduce recidivism. Job titles vary widely , some departments advertise for "mental health professional in law enforcement," others for "community resource specialist" , but all share a core of crisis assessment, de-escalation, and linkage to care. In Pittsburgh's latest model, mental health clinicians are stationed at police headquarters and pair with officers across all zones, showing how embedded positions are becoming structured, permanent roles rather than grant-funded pilots. Social workers considering this path should also review the broader landscape of forensic social work to understand how criminal justice settings shape scope of practice.
Salary and Pay Scales in Pennsylvania
Pay for law enforcement-social work hybrids is less standardized than hospital or school social work. Data specific to co-response roles is not yet systematically published, but broader state figures offer a baseline. The U.S. Bureau of Labor Statistics reports that child, family, and school social workers in Pennsylvania earn a median annual wage of approximately $50,000, while "social workers, all other" , a category that often includes those in criminal justice settings , earn closer to $60,000. Forensic and crisis-focused social workers employed by counties or municipalities tend to fall in the $55,000 to $70,000 range depending on licensure and experience. Positions embedded in police departments may carry higher salaries than community agency roles, sometimes reaching $75,000 or more, particularly for LCSW-level clinicians with specialized CIT training. When evaluating a co-response job, look beyond the base salary: some municipalities offer hazard pay, flexible schedules, and public pension benefits that significantly increase total compensation.
Qualifications: MSW, LCSW, and CIT Training
Almost all police-based social work positions require at least a Master of Social Work (MSW) degree from an accredited program. The Licensed Clinical Social Worker (LCSW) credential is strongly preferred for independent practice, especially in roles that involve diagnostic assessment or psychotherapy on scene. Some entry-level co-response or victim advocate jobs accept a Licensed Social Worker (LSW) who works under clinical supervision, but the trend is toward full licensure. Crisis Intervention Team (CIT) training , a 40-hour curriculum that teaches de-escalation, mental health recognition, and officer safety , is increasingly listed as a prerequisite or required within the first year of hire. Familiarity with motivational interviewing, trauma-informed care, and substance use disorder treatment also strengthens an application. Candidates who want to deepen their expertise before entering the field may find value in exploring post-MSW clinical fellowship programs that focus on high-acuity or justice-involved populations.
How MSW Programs Prepare You for Law Enforcement Settings
The clearest path into this field is through a field placement with a police department, sheriff's office, or mobile crisis unit during an MSW program. Not all schools offer such placements, so students should specifically inquire about forensic, criminal justice, or crisis intervention practicum sites. Coursework in forensic social work, policy advocacy, crisis intervention, and psychopathology builds the clinical foundation, while interprofessional simulations with criminal justice students help develop the communication skills needed when working alongside officers. Programs that emphasize macro practice or administrative leadership are also valuable, as co-response teams often require navigating complex funding streams and interagency agreements. After graduation, many social workers seek out advanced certificates in trauma-focused therapy or psychiatric rehabilitation to further specialize.
Common Questions About Police-Social Worker Co-Response Teams
As police-social worker partnerships evolve, practitioners often ask how these teams function and what they require. Below are concise answers to common questions, with references to detailed sections throughout this article.