Points of interest…
- Suicide accounts for 56 percent of U.S. gun deaths, making lethal means counseling a core social work competency.
- Most employers ban firearms on premises, so social workers rarely carry guns regardless of state carry laws.
- A structured five step firearm risk assessment moves from screening questions through safe storage planning to documentation.
- Six evidence based intervention models, including Cure Violence and hospital based programs, place social workers in leadership roles.
Gun violence claimed 46,728 lives in the United States in 2023, a toll that places the issue squarely in social work's domain. Yet most MSW programs never require students to practice a firearm risk assessment, and only a fraction of social work employers provide formal training in lethal means counseling.
Gun violence is a public health crisis that intersects with every social work domain: mental health social work, child welfare, community organizing, and criminal justice reform. The gap between what the field demands and what training provides has real consequences for client outcomes and practitioner safety. This guide walks through the data social workers need, the assessment protocols that should be standard practice, the intervention models where the profession leads, and the training pathways available right now.
Gun Violence as a Public Health Crisis: The Numbers Social Workers Need to Know
In 2023, the United States recorded 46,728 firearm-related deaths, with suicides accounting for 56 percent and homicides 40 percent.1 The remaining deaths involve law enforcement, unintentional shootings, and undetermined circumstances. An estimated 84,600 nonfatal firearm injuries occur annually, with roughly 70 percent resulting from assaults and 20 percent from unintentional discharges.2 For children and teens ages 1 to 19, firearm injuries surpassed motor vehicle crashes as the leading cause of death in 2022, claiming an average of 2,345 young lives each year.3 These numbers frame gun violence as a public health emergency that touches every corner of social work practice, from school social worker roles to crisis intervention.
The Suicide Majority: A Misunderstood Crisis
When most people think of gun violence, community violence and mass shootings dominate the narrative. In reality, nearly three out of five firearm deaths are suicides.1 Social workers encounter suicidal ideation far more frequently than they encounter overt violence, whether in clinical mental health settings, emergency departments, or child welfare social worker visits. The sheer volume of suicide-by-firearm means that routine depression screens, safety plans, and lethal-means counseling are frontline prevention tools, yet many practitioners still underestimate the role of firearms in completed suicides. Recognizing this ratio is essential for every social worker conducting psychosocial assessments.
Deep Disparities Along Racial and Geographic Lines
The burden of gun violence is not distributed evenly. Black Americans are 13 times more likely to die by gun homicide than white Americans, and Hispanic Americans are twice as likely.3 Black boys and men, who represent just 6 percent of the U.S. population, account for 52 percent of all gun homicide victims. Among children and teens, Black youth are 16 times more likely to be killed by a firearm than their white peers, a disparity that has persisted since at least 2006.3 Meanwhile, rural communities experience elevated rates of suicide-by-firearm, driven by firearm access, social isolation, and limited mental health infrastructure. These patterns mean that social workers in urban hospitals, rural clinics, and community-based agencies each confront distinct firearm risks shaped by place and race.
Upstream Drivers: Why Gun Violence Is a Social Issue
Gun violence is not solely a criminal justice or public safety problem. It is deeply rooted in the social determinants that social workers tackle daily. Poverty, housing instability, childhood trauma, under-resourced schools, and economic disenfranchisement all correlate with higher firearm injury rates.2 When a client cannot afford rent, lives in a neighborhood with elevated violence, or lacks access to mental health care, the risk of experiencing or perpetrating gun harm rises. This is why social work's person-in-environment perspective is indispensable: effective prevention demands addressing the upstream factors that make firearms lethal in the first place. Viewing gun violence as a social issue, not just a law enforcement one, opens the door for social workers to lead in community social work interventions, policy advocacy, and equitable resource distribution.
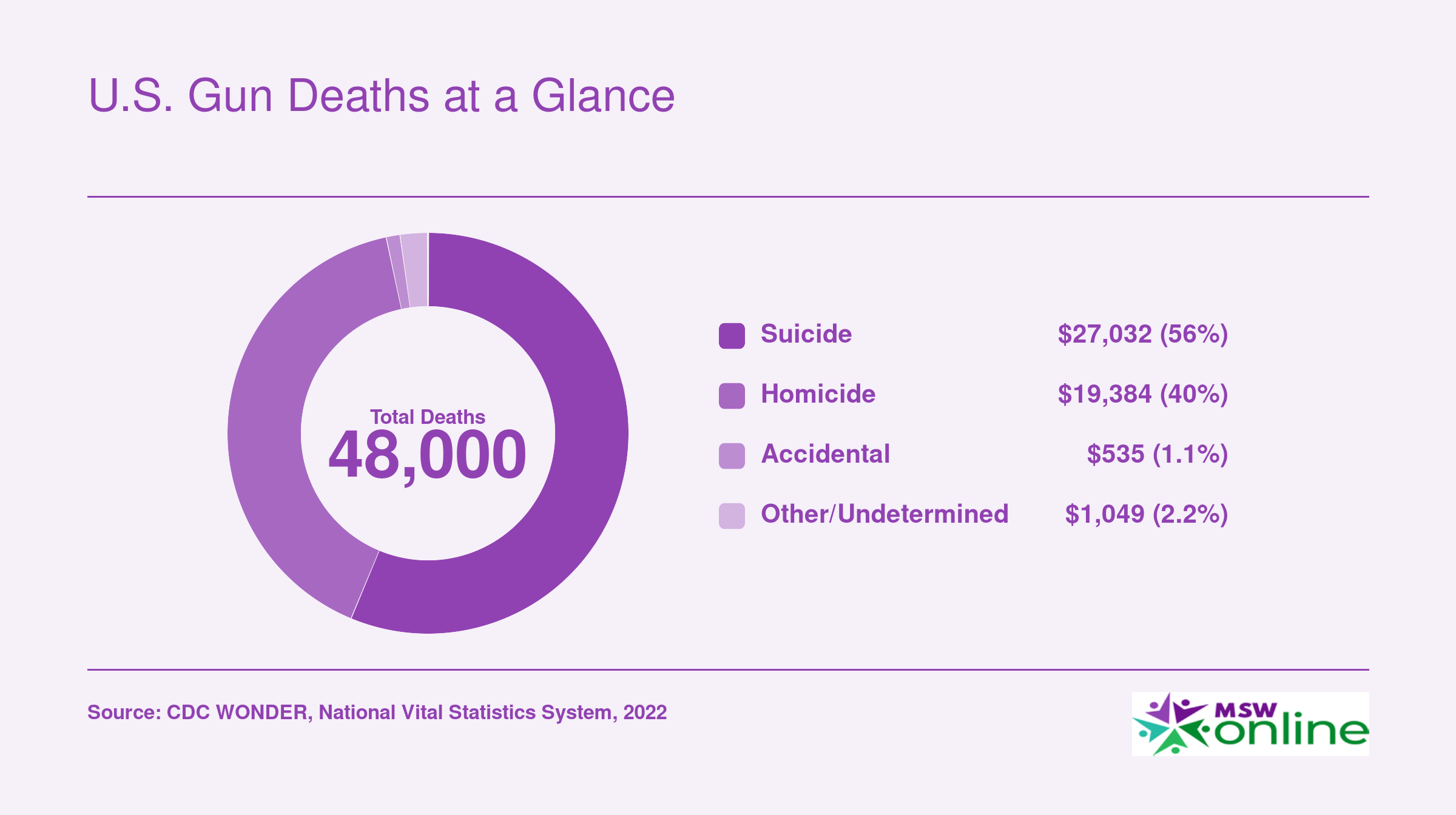
U.S. Gun Deaths at a Glance
Gun violence claims tens of thousands of lives in the United States each year. Understanding how those deaths break down by cause is essential for social workers designing targeted prevention strategies. Suicide consistently accounts for the largest share, a fact that underscores the profession's critical role in mental health screening and safe-storage counseling.
The Role of Social Workers in Gun Violence Prevention, by Setting
Gun violence prevention doesn't happen in one place or through one profession. Social workers are effective in this space precisely because they operate across systems, connecting clinical assessment to community resources to policy advocacy in ways that no single other discipline does. The NASW classifies gun violence as a major public health crisis and explicitly supports social worker engagement in prevention as a professional duty, including advocacy for background checks, red flag laws, and safe storage policies.1
Hospitals and Emergency Departments
When a gunshot wound patient arrives in an emergency department, a physician treats the injury. The social worker does something different: they conduct a trauma-informed psychosocial assessment at the bedside, screen for retaliation risk and ongoing violence exposure, and connect the patient to community partners before discharge.2 Hospital-based violence intervention programs (HVIPs) rely on social workers to coordinate this post-discharge wraparound care. Without that coordination, a patient returns to the same environment that produced the injury in the first place. Social workers are frequently the only members of an HVIP team with both the clinical licensure to assess mental health needs and the case management skills to act on them.
Schools
School social workers sit on multidisciplinary threat assessment teams, contributing something distinct from what school counselors or psychologists provide: a broad assessment of a student's mental health, social supports, violence exposure, and family context, plus the capacity to engage families directly in the response.3 That family-engagement function is the gap school social workers fill in threat assessment. They also lead crisis intervention and recovery efforts after incidents occur.4 The Multi-Tiered System of Support framework positions school social workers to deliver counseling, conflict resolution, and anger management services across all three tiers of student need. Advocacy tied to the School Social Workers Improving Student Success Act centers on lowering student-to-social worker ratios, a staffing reality that directly limits prevention capacity.3
Community-Based Organizations
In community violence intervention (CVI) programs, social workers collaborate with street outreach workers and credible messengers, handling the case management, mental health, and family support functions that outreach workers are not trained to provide.1 CVI programs target the small percentage of individuals at the highest risk of shooting or being shot. Social workers integrate those individuals into services addressing the root causes of violence: poverty, unemployment, and housing instability.
Clinical and Private Practice
In outpatient and private practice settings, the gun violence prevention role is quieter but no less consequential. Social workers conduct suicide risk screenings and provide lethal means counseling, which means directly discussing firearm access with clients at elevated risk. Professionals pursuing trauma certifications for social workers can deepen their competency in these high-stakes conversations. The Grand Challenges for Social Work initiative named preventing gun violence as one of its core goals5, and curriculum guidance from social work educators now recommends that all clinical training include prevention, trauma-informed care, policy advocacy, and multidisciplinary collaboration as foundational competencies.4
Across every setting, the social worker's function is connective: bridging the space between what a clinical assessment reveals and what a community can actually provide.
Can Social Workers Carry Guns?
Can social workers carry guns? The direct answer: there is no blanket federal law prohibiting licensed social workers from carrying firearms. However, in practice, the vast majority of social work employers, including hospitals, schools, government agencies, and nonprofit clinics, ban weapons on premises. Carrying a firearm while in direct client contact raises serious ethical and liability concerns that make it effectively off-limits for most practitioners.
The Legal Reality: Employer Policies Override Personal Rights
Though some states have permissive concealed-carry laws, most social work employers have workplace weapons policies that prohibit firearms. Even if a social worker has a legal permit to carry, bringing a weapon into an agency office, a client's home, or a school-based setting typically violates policy and can result in immediate termination or licensure investigation. During home visits, the client's private property may also have its own restrictions. Federal buildings, such as VA hospitals or tribal agencies, impose additional bans. Always check both state law and your employer's handbook before considering carrying.
Ethical Guidance from the NASW Code of Ethics
The NASW Code of Ethics does not explicitly mention firearms, but its core principles create strong ethical guardrails. The duty to "do no harm" (1.04) and respect client self-determination (1.02) mean that introducing a weapon into a therapeutic relationship risks undermining trust and safety. A social worker's primary role is to de-escalate and promote a sense of security; the visible or known presence of a firearm can escalate tensions, particularly with clients who have trauma histories or paranoia. Additionally, the standard of care (1.04) requires that interventions not create foreseeable risk. Carrying a gun in volatile situations may increase liability if an incident occurs.
Distinguishing Personal Rights from Professional Practice
A social worker may legally own firearms for personal protection or recreation, but exercising that right while on duty is a separate matter. The distinction is crucial: your concealed-carry permit does not override employer policies or the ethical responsibilities inherent in your professional role. Social workers in settings like forensic social work encounter high-risk situations regularly, yet even these practitioners are bound by agency safety protocols rather than personal armament. Many agencies have clear "no weapons" policies that apply regardless of off-duty habits. If you feel unsafe, the constructive approach is not to arm yourself but to rely on structured safety procedures.
Safer Alternatives: Building Personal Safety Without Firearms
Social workers concerned about personal safety, especially those conducting home visits or working in high-crime areas, should advocate for employer-provided safety measures. De-escalation training, buddy systems, check-in procedures, and conflict resolution skills are evidence-based interventions that reduce risk without introducing weapons. The upcoming section on social worker safety details these protocols. Carrying a gun is not a substitute for a comprehensive workplace safety plan.
Questions to Ask Yourself
Firearm Risk Assessment Protocols for Social Workers: A Step-By-Step Framework
Asking a client about firearms can feel more intrusive than asking about medications, sleep habits, or household chemicals, yet the clinical rationale is identical: you are screening for access to lethal means in a person who may be at risk. Framing the inquiry as a standard safety practice, not a political statement, helps both the practitioner and the client engage honestly. The five-step sequence below draws on the SAFE-T protocol paired with the Columbia Suicide Severity Rating Scale (C-SSRS) and the Counseling on Access to Lethal Means (CALM) framework.1
Step 1: Universal Screening Question at Intake
Every intake, regardless of presenting concern, should include at least one brief screening question about suicidal ideation. The C-SSRS screening version works well here because it differentiates between ideation, plan, and intent in just a few questions.1 At this stage you are not singling anyone out; you are casting a wide, non-judgmental net. If the client screens negative, you document the result and move on. If any level of ideation is endorsed, you proceed to Step 2.
Step 2: Follow-Up Lethal Means Inquiry
Once risk is identified, shift to a direct lethal means conversation. The SAFE-T protocol explicitly instructs clinicians to ask about the presence or absence of a firearm in the home or workplace, as well as ease of access.2 CALM provides a conversational structure for this moment: acknowledge the client's distress, explain why you are asking about means, and use open-ended prompts. You are not interrogating; you are partnering with the client to reduce danger. Practitioners who work with veterans or service members in particular, such as those pursuing military social work, should be prepared for strong cultural attitudes toward firearm ownership and tailor their approach accordingly.
Step 3: Assessment of Access
Dig deeper into specifics. Who owns the firearm? Where is it stored? Is it locked, and who has the key or combination? Are ammunition and the firearm stored separately? These details matter because research consistently shows that time and barriers between a person in crisis and a loaded weapon reduce lethality. The Columbia Risk and Protective Factors checklist explicitly includes access to lethal means as a risk factor.2 Note that "access" extends beyond ownership: a client who does not own a gun but can easily borrow one from a family member still has meaningful access.
Step 4: Risk Stratification Using Validated Tools
Combine what you have gathered into a structured risk level. The SAFE-T with C-SSRS uses three tiers (low, moderate, high) and requires documentation of the risk level, the clinical rationale behind it, the interventions selected, and a follow-up plan.2 The C-SSRS itself flags preparatory behaviors, such as acquiring a firearm, as indicators that elevate risk beyond ideation alone.3 Using a validated instrument protects the client and also gives you a defensible clinical record.
Step 5: Documentation Standards and Escalation Triggers
Your chart entry should capture a clear chain of reasoning:
- Screening tool used: Name the instrument (e.g., C-SSRS screener) and record the client's responses.4
- Firearm-specific findings: Note presence, ownership, storage method, and accessibility without editorializing.
- Risk level and rationale: State the tier and the factors that led to that classification.
- Interventions: Record what you did, whether that was a safety plan, a voluntary storage agreement, a referral, or an emergency hold.
- Follow-up plan: Specify the timeline and responsible party for re-assessment.
When documenting firearm access, chart only what is clinically relevant. A client's legal gun ownership is not, by itself, a clinical concern; its intersection with acute risk is. This distinction respects both confidentiality expectations and the therapeutic relationship.
Mandatory reporting triggers vary by jurisdiction, but in general you must act when there is an imminent, identifiable threat to a specific person (duty to warn) or when the client is an imminent danger to themselves and refuses voluntary safety measures. Know your state's statutes before you sit down with a client, not after. Staying current on legal requirements is one reason continuing education for social workers matters throughout your career.
Treating the firearm question as routine rather than extraordinary is the single most important shift a practitioner can make. When every client hears the same intake screen, no one is singled out, and the conversation about means becomes just another part of competent clinical care.
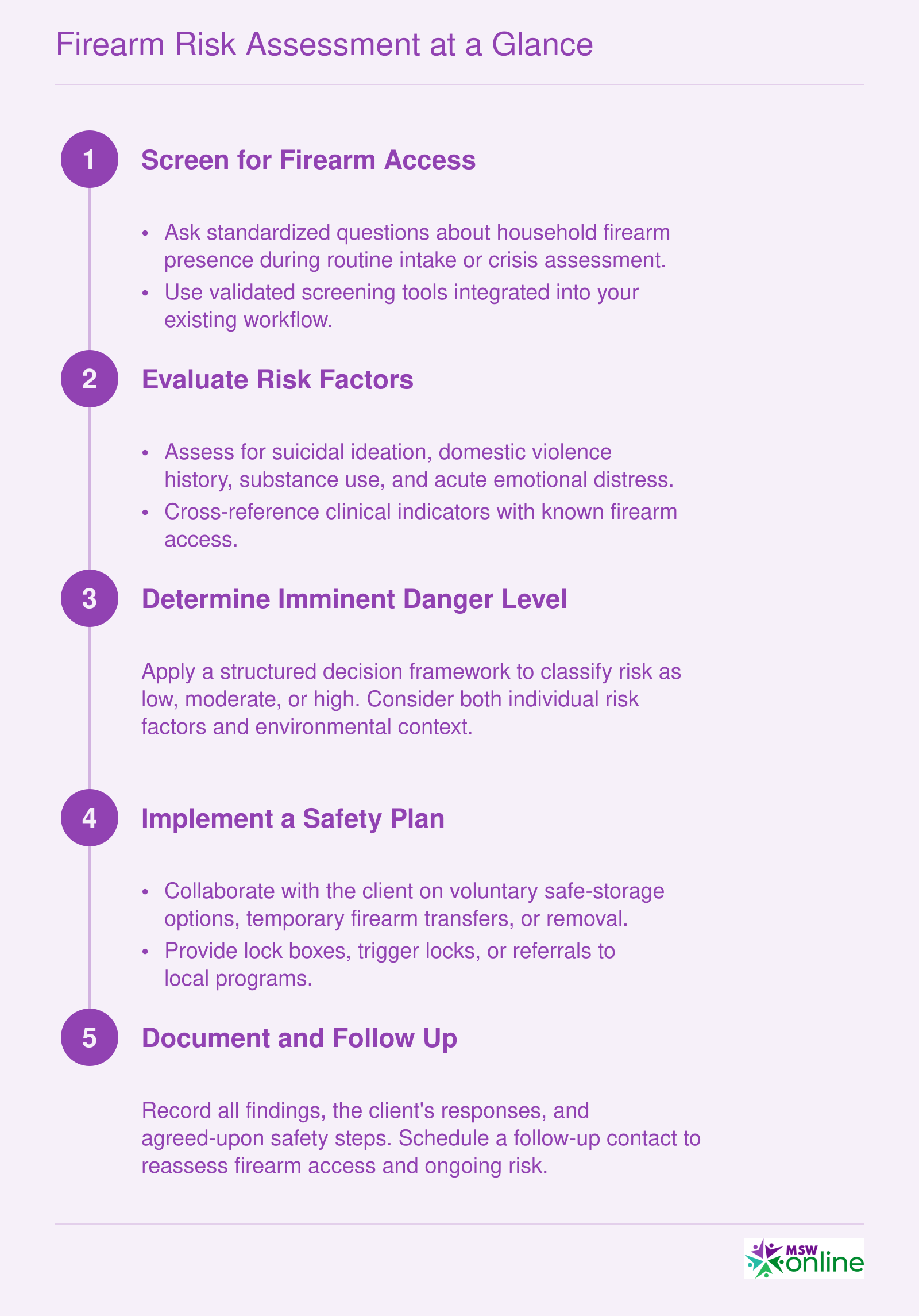
Firearm Risk Assessment at a Glance
This framework distills the structured firearm risk assessment process into five ordered steps. Each stage builds on the previous one, guiding practitioners from initial screening through safe resolution and documentation.
Safe-Storage Counseling: Scripts, Tools, and Ethical Guardrails
Firearm storage counseling is moving from an optional add-on to a standard-of-care expectation for social workers in broad practice settings. Clinicians now have an expanding toolkit of scripts, community resources, and ethical frameworks to integrate lethal-means safety into routine conversations without alienating clients or overstepping professional boundaries.
Scripts and Language That Work
The Counseling on Access to Lethal Means (CALM) training, available free online through the Suicide Prevention Resource Center (SPRC) and the Means Matter campaign, provides concrete, non-confrontational scripts. The emphasis is on temporary, voluntary storage changes during high-risk periods, framed as a safety collaboration rather than a rights infringement. Downloadable clinician guides model phrasing such as "Many families I work with find it helpful to store firearms outside the home for a time when someone is struggling" and "Would you be open to talking about steps that could add a layer of protection?" The CALM approach encourages clinicians to first ask about the presence of firearms in the same neutral tone they use when asking about other safety hazards, then to explore storage options only if the client is receptive. Practice scripts for different scenarios (homes with adolescents, older adults with cognitive decline, individuals in acute crisis) can be found in the accompanying clinician pocket guides.
Free Gun Locks and Community Partnerships
A practical bridge between counseling and action is the distribution of free cable-style gun locks through Project ChildSafe. The program's official website lists local law enforcement partners, and many police departments and sheriff's offices give locks away with no questions asked. Social workers can connect clients to these resources directly or maintain a small supply in their agency for immediate use. Pairing a lock handout with a brief demonstration and the CALM conversation normalizes storage modifications as a routine safety practice.
Guides Tailored to Social Work Practice
Beyond CALM, the National Association of Social Workers (NASW) practice resources and the American Counseling Association (ACA) firearm safety toolkits offer structure specifically for mental health and social service settings. These guides address documentation, informed consent nuances, and how to collaborate with families on storage agreements. They also include checklists for assessing storage hazard (loaded, unlocked, accessible ammunition) and templates for "means-restriction safety plans" that document where firearms will be stored and who holds the keys. Practitioners seeking additional credentials in this area may want to explore social work certifications that include crisis-intervention or safety-planning competencies.
Legal and Ethical Guardrails
Safe-storage counseling sits at the intersection of client self-determination and duty to protect. Social workers must review their state's duty-to-warn statutes; some mandate reporting if a client makes a credible threat and has access to a firearm, while others only permit such disclosure. Scope-of-practice guidelines from your licensing board clarify whether you can physically assist with storage arrangements or merely counsel and refer. The APA and NASW ethics codes underscore that safety interventions must be the least intrusive necessary and that the client's cultural context regarding firearms should be respected. For a deeper overview of these principles, see our guide to social work ethics. In practice, this means asking permission before discussing storage, avoiding ultimatums, and documenting the conversation as a collaborative safety measure, not a confiscation directive.
- State duty-to-warn: Check your licensing board for current requirements; some states explicitly include firearm access in the threat assessment.
- Documentation: Note the client's willingness to engage, the specific storage plan agreed upon, and any follow-up steps.
- Cultural competence: Frame storage counseling within the client's values (e.g., family safety, responsibility) rather than a political debate.
Safe-storage counseling is not about gun politics. It is a clinical harm-reduction strategy with the same logic as asking about seatbelts, medication storage, or pool fences. Frame it that way to clients and to yourself.
Intervention Models Where Social Workers Lead
Social workers do not simply participate in gun violence reduction efforts. In several well-established intervention models, they occupy leadership and direct-service roles that are central to program design, delivery, and evaluation.1 The table below compares six models, spotlighting where social workers fit and what the outcome evidence shows.
Model Comparison
| Model | Social Worker Role | Primary Population | Notable Outcome |
|---|---|---|---|
| Community Violence Intervention (CVI) Programs | Clinical directors, therapists, case managers, and policy advocates who shape program strategy and deliver direct services | Individuals at highest risk of shooting or being shot | 15 to 40 percent reduction in shootings and homicides across implementation sites |
| Hospital-Based Violence Intervention Programs (HVIPs) | Hospital-embedded social workers providing crisis intervention, case management, outpatient follow-up, and family support at the bedside | Violently injured patients (gunshot and stabbing survivors) reached during the "teachable moment" | 30 to 50 percent reduction in repeat violent injury; 20 to 40 percent reduction in arrests |
| Cure Violence Street Outreach | Clinical supervisors, case managers, trauma and grief counselors, and program evaluators who guide outreach staff | High-risk individuals in neighborhoods with concentrated violence, using a public-health contagion framework | Greater than 30 percent decrease in shootings and killings; an estimated $18 saved for every $1 invested |
| Group Violence Intervention (GVI / Focused Deterrence) | Lead service coordinators, case managers, family clinicians, and interagency liaisons connecting participants to resources | Small groups of individuals at highest risk for shooting or being shot | Greater than 30 percent decline in shootings with injuries across many implementations |
| Advance Peace | Program leadership, life coaching, and clinical support to fellowship coaches working with the most at-risk individuals | Individuals identified as being at the very highest risk | 20 percent reduction in homicides and non-fatal shootings in Sacramento (2018 to 2019); $18 to $41 saved per $1 invested |
| School-Based Threat Assessment Teams | Licensed clinical social workers serving on multidisciplinary teams that evaluate student threats, coordinate safety plans, and connect families to services | Students who have made threats or exhibited warning behaviors in K-12 settings | Emerging evidence supports reduced disciplinary removals and safer school climates when teams follow structured protocols |
Why the Social Work Lens Matters
Many overviews of these models focus on program architecture, funding streams, or law enforcement partnerships. What often gets lost is the clinical and relational work that makes each model function. In HVIPs, for example, a social worker at the bedside within hours of a shooting transforms a medical encounter into a turning point.2 In CVI programs, social workers design trauma-informed service plans that address housing instability, substance use, and mental health, not just the immediate risk of retaliation.1
Choosing a Path
If you are drawn to one of these models, your entry point depends on your degree level and licensure status. BSW-level practitioners often start as case managers or outreach staff within CVI or Cure Violence programs. MSW-prepared clinicians move into supervisory, clinical director, or program evaluation roles, and some may eventually pursue careers in social work that span multiple intervention settings. Across every model, the throughline is the same: social workers bring person-in-environment thinking, trauma-informed practice skills, and a commitment to racial equity that distinguishes these interventions from purely law enforcement or public health approaches. Practitioners interested in school-based threat assessment teams may also benefit from completing a school social work certification to strengthen their credentials.
The evidence base for these models continues to grow. The resources listed below from the Vera Institute of Justice, Johns Hopkins Center for Gun Violence Solutions, and LISC provide deeper dives into implementation specifics and funding landscapes for practitioners ready to get involved.3
Social Worker Safety and Workplace Violence: What the Data Shows
The Bureau of Labor Statistics recorded 5,070 fatal work injuries across all U.S. occupations in 2024, a figure that underscores the broader context in which social worker safety must be understood.1 While that total spans every industry, the social services sector consistently registers workplace violence rates well above the national average, and practitioners need to know exactly where to find reliable data so they can advocate for safer conditions.
Where to Find Federal Data
Two BLS programs are your starting point. The Census of Fatal Occupational Injuries (CFOI) publishes annual fatality counts broken down by occupation code. Social workers fall under the SOC 21-1020 series; searching that code on BLS.gov surfaces year-by-year fatal injury totals specific to the profession.3 The Survey of Occupational Injuries and Illnesses (SOII) complements those numbers with nonfatal assault rates, giving you a fuller picture of how often social workers experience violence that results in missed workdays or job transfers.
For context, the total recordable case rate for all private-industry workers was 2.3 per 100 full-time equivalent employees in 2024.2 Social services occupations have historically exceeded that benchmark, sometimes by a wide margin, but the precise ratio shifts from year to year. Pulling the most current SOII tables lets you make an apples-to-apples comparison.
OSHA's website adds another layer. Its enforcement case database and industry-specific reports document violations and inspections in social service settings. Comparing those findings against national averages can reveal whether your employer or practice environment is an outlier.
Professional Association Surveys
Federal datasets capture reported incidents, but many workplace threats go unreported. The National Association of Social Workers (NASW) and the Council on Social Work Education (CSWE) periodically publish member safety surveys that capture a broader range of experiences, from verbal threats to stalking. These reports often include best-practice recommendations for agency-level safety policies. Check the research and publications sections of both organizations' websites for the latest releases. Practitioners pursuing advanced credentials through forensic social work certification programs may find these survey findings especially relevant to their specialty.
Localized and Program-Level Data
National figures may not reflect what is happening in your city or state. For more granular information:
- State licensing boards: Some boards track complaints and incidents involving practitioner safety and may share aggregate data on request.
- University social work programs: Schools with active research agendas sometimes conduct their own workplace violence surveys among alumni and field placement students.
- State OSHA plans: States that operate their own occupational safety programs may publish enforcement and injury data that drill down further than the federal datasets.
Reaching out directly to these bodies takes effort, but the localized picture they provide is often more actionable than national averages when you are evaluating a specific job offer or pushing for policy changes at your agency.
Turning Data Into Action
Knowing the numbers is only useful if it changes practice. Use federal and association data to benchmark your workplace, support budget requests for safety measures like panic buttons or buddy systems for home visits, and hold employers accountable to OSHA's General Duty Clause. If your agency lacks a written workplace violence prevention plan, the data you gather becomes the foundation for building one.
Social workers experience nonfatal workplace violence at a rate 10 to 15 times higher than the average U.S. worker, according to Bureau of Labor Statistics data from 2021–2022. This elevated risk underscores the critical need for safety protocols, violence-prevention training, and institutional support in social work settings.
Training Pathways and Continuing Education in Gun Violence Prevention
Where can a social worker actually get trained in gun violence prevention, and what does that training look like in practice?
What MSW Programs Currently Offer
Dedicated gun violence content remains rare at the BSW and MSW levels. Most programs have not built stand-alone courses on firearm injury prevention into their curriculum. Where the topic does appear, it tends to be embedded inside trauma, crisis intervention, or social policy courses, sometimes as a single module or case study rather than a sustained focus.
A small number of schools of social work have begun developing electives or certificate tracks connected to community violence intervention, and some public health-oriented MSW programs address firearms within broader injury prevention frameworks. But as of 2026, no MSW program has gained widespread recognition specifically for a gun violence concentration the way some programs are known for military social work or health policy. If you are selecting a program and this is a priority, ask admissions staff directly which courses address lethal means, firearm risk, or community violence. Students drawn to trauma-focused practice may also want to explore social work trauma certification options that complement gun violence coursework.
The CALM Training: The Most Actionable Step Available Now
For practitioners already in the field, the single highest-impact training available is Counseling on Access to Lethal Means, commonly called CALM. The Suicide Prevention Resource Center offers a free online CALM course that takes approximately two hours to complete.1 It is open to mental health professionals, social service professionals, and health care providers, and requires a post-test score of at least 80 percent along with a feedback survey to receive a certificate of completion.1
Note that the SPRC online course does not currently carry continuing education credit on its own.1 If CE credit matters for your license renewal cycle, Psych Hub offers a CALM course approved for 2.25 CE hours for social workers through the NASW-New Jersey Social Work Continuing Education Approval Collaborative, with that approval running through August 31, 2026.2 AgriSafe Network also offers a CALM-based training with CE credit available for community health workers and Louisiana licensed professional counselors.3
For organizations wanting more intensive training, CALM America offers a clinical workshop running 3.5 to 4 hours, a 90-minute CALM-SAFE format, a day-long Lethal Means Academy, and a Train-the-Trainer program for agencies building internal capacity.4
NASW, CSWE, and the Broader CE Landscape
NASW has published position statements on gun violence and offers some continuing education through its Learning Center, though CE courses focused specifically on firearm risk assessment or lethal means counseling are not yet a standard part of the catalog. CSWE's Educational Policy and Accreditation Standards address trauma, crisis, and community practice broadly but do not single out gun violence as a named competency domain at this time.
This gap is worth naming directly: the professional infrastructure for gun violence training in social work is still developing. That is not a reason to wait.
A Practical Path Forward
Social workers do not need to hold out for their program or employer to add gun violence content before building competency. Start with the free SPRC CALM course this week. If CE credit is needed, explore the Psych Hub version before its current approval window closes. Those interested in clinical MSW programs should ask prospective schools whether their curriculum addresses lethal means counseling. Advocate within your program or agency for curriculum and training that addresses lethal means explicitly. The tools exist now. The gap is mostly organizational inertia, and practitioners can move faster than institutions.
Common Questions About Social Work and Gun Violence
Gun violence intersects with nearly every area of social work practice, from clinical assessment to community organizing. Below are answers to the questions practitioners and students ask most often, drawn from the frameworks and data covered throughout this guide.
Gun violence competency is not a specialty credential you earn once and file away. It is a set of practical skills, from screening for firearm access to counseling on safe storage, that belongs in everyday social work practice.
Three steps you can take right now: First, complete the free CALM (Counseling on Access to Lethal Means) training this week. It takes roughly two hours and directly sharpens the lethal-means conversations covered earlier in this guide. Second, ask your agency whether a formal firearm risk assessment protocol exists. If it does not, bring the step-by-step framework from this article to your supervisor as a starting point. Third, identify a Community Violence Intervention or Hospital Violence Intervention Program near you and clarify the referral pathways before you need them.
With more than 46,000 firearm deaths recorded in 2023, the scale of this crisis puts it squarely within social work's public health mandate. Whether you are pursuing social work in mental health or community practice, prevention is not a niche interest. It is becoming a core competency.
Explore More
- Bilingual Social Worker
- Continuing Education for Social Workers
- COVID-19 Guide for Social Workers
- CSWE Accreditation
- DSW vs. PhD in Social Work
- Environmental Social Work
- Free Implicit Bias Tests & Training Resources
- How Long Does It Take to Become a Social Worker?
- How Social Work Reduces Healthcare Costs
- How to Find a Social Work Job
- Levels of Social Work Licensure
- LGBTQIAP in Social Work
- Mental Health & Homelessness
- Micro, Mezzo & Macro Social Work
- MSW Admission Requirements
- MSW Scholarships
- MSW Specializations
- MSW vs. MSSW
- Remote Resources for Mental Health Workers
- Social Work & Food Insecurity
- Social Work Ethics
- Social Work Field Placement Guide
- Social Work Grants
- Social Work Internships
- Social Work Theories & Practice Models
- Social Work Volunteer Opportunities
- Social Work vs. Counseling
- Social Work vs. Psychology
- Social Work vs. Sociology
- Social Worker Salary Guide
- Social Worker vs. Therapist
- Social Worker's Guide to Cyberbullying
- Student Mental Health & Social Work on College Campuses
- What Can You Do With an MSW Degree? Careers & Salaries
- Why Is Research Important in Social Work? A Complete Guide
- Women in Social Work Leadership