Points of interest…
- Over 80 percent of the one billion women in or approaching menopause experience depression, anxiety, or cognitive changes.
- FamilyWell Health's new Menopause Behavioral Health Certification offers accredited continuing education credits specifically for social workers.
- CBT adapted for menopause is the strongest evidence-based psychosocial intervention social workers can deliver without a prescribing license.
- Healthcare social workers and mental health social workers both hold faster than average job growth through the current decade.
When a 48-year-old woman presents with new-onset anxiety and insomnia, a primary care physician often prescribes an SSRI and sleep hygiene guidance. A social worker trained in menopause-informed care recognizes a different pattern: vasomotor symptoms disrupting sleep, cognitive fog shaking professional confidence, and role strain spilling into family life. The difference matters because over 1 billion women worldwide are in or approaching menopause, and more than 80% experience symptoms that include depression, anxiety, cognitive changes, and sleep disruption.1
Menopause is not a narrow endocrinological event. It lands squarely at the intersection of role transition, occupational disruption, and the social determinants that shape how midlife women access care, maintain employment, and hold households together. Yet psychiatric social work training programs rarely address it.
With fewer than 10% of workplaces maintaining menopause policies and most clinical curricula silent on the subject, social workers who build expertise now enter an open field where their psychosocial lens is the missing piece.
Why Menopause Is a Social Work Concern
Menopause is the permanent cessation of menstrual periods, diagnosed after twelve consecutive months without a cycle, typically occurring between ages 45 and 55. Perimenopause, the transition phase that precedes it, can last four to ten years and brings unpredictable hormonal fluctuations that affect mood, cognition, sleep, and physical health. For social workers, menopause is not simply a medical event but a biopsychosocial transition embedded in a web of roles, relationships, systems, and inequities.
The Person-in-Environment Lens
Social work's person-in-environment perspective sets the profession apart in menopause care. Social work vs. psychology distinctions matter here: while psychiatrists manage neurochemical imbalances and psychologists deliver individual therapy, social workers assess the full ecological context, including a client's caregiving burden for aging parents or adolescent children, financial stress from stalled career mobility or medical costs, relationship strain as intimacy and communication shift, and workplace ageism that marginalizes women over 50. Hormonal mood changes do not occur in a vacuum. They interact with chronic stress, role overload, and systemic barriers, amplifying distress and impairing function. Social workers are trained to see these intersections and intervene at multiple levels, from micro (individual coping) to mezzo (family dynamics) to macro (policy advocacy).
Social Determinants of Health and Menopause Disparities
Access to menopause care varies sharply by race, income, insurance status, and geography. Black and Latina women report more severe vasomotor symptoms (hot flashes, night sweats) and higher rates of depressive symptoms during perimenopause than white women, yet they receive hormone therapy and mental health treatment at lower rates. Rural women face geographic barriers to specialists, and uninsured or underinsured women often forgo care entirely. Social workers routinely address these social determinants, connecting clients to affordable care, advocating for coverage, and designing interventions that account for cultural beliefs and structural barriers.
Midlife Role Strain and the Sandwich Generation
The menopause window coincides with peak midlife role strain. Many women in their late forties and fifties provide care for aging parents while still supporting children financially or emotionally, a phenomenon known as sandwich caregiving. Simultaneously, careers may plateau or face forced exits due to age discrimination. Identity shifts accompany physiological changes as women renegotiate self-concept around fertility, sexuality, and aging. These stressors compound the mood disruptions triggered by fluctuating estrogen and progesterone, creating a convergence of risk that geriatric social workers and other midlife-focused practitioners are uniquely positioned to address.
The Training Gap
Social workers are already embedded in the settings where menopausal clients present: community mental health centers, hospital discharge planning units, employee assistance programs, primary care clinics, and integrated behavioral health teams. Yet most receive no menopause-specific training in their MSW programs or continuing education. The result is missed opportunities for early screening, psychoeducation, and tailored intervention. Closing this gap is both a clinical imperative and a professional development opportunity.
Mental Health Risks During Perimenopause and Menopause
The clinical understanding of menopause-related mental health has shifted considerably in recent years, yet a significant gap persists between what research reveals and what most behavioral health providers are trained to recognize. For social workers conducting intake assessments or managing ongoing caseloads, understanding the specific psychiatric risks of the menopause transition is not optional; it is foundational to competent practice.
Core Psychiatric Risks
Perimenopause, the phase when hormone fluctuations are most erratic, carries the highest mental health burden. Common presentations include new-onset depression, generalized anxiety, irritability that disrupts relationships and work functioning, persistent insomnia, and a cognitive fog often described by clients as difficulty concentrating or "losing words." Suicide risk also rises during this window, particularly among individuals with no prior psychiatric history who may not be identified through standard risk-screening protocols.
Women who have experienced premenstrual dysphoric disorder, postpartum depression, or earlier depressive episodes face heightened vulnerability. For these individuals, the hormonal volatility of perimenopause can reactivate or intensify mood symptoms that had been stable for years, sometimes decades. Social workers should treat any history of hormonally linked mood disruption as a meaningful risk factor during midlife assessment.
Intersectional and Racial Disparities
Menopause does not affect all populations equally. Data from the Study of Women's Health Across the Nation (SWAN) and related research show that Black women enter menopause roughly 8.5 months earlier on average than white women1 and experience vasomotor symptoms at higher rates (46 percent compared to 37 percent for white women).1 Depressive symptoms during the transition are also more prevalent among Black women (27.4 percent versus 22.3 percent), and the rate of new-onset depression is markedly higher (20 percent versus 13 percent).2
Despite greater symptom burden, Black women are far less likely to receive treatment. Only 43 percent of Black women experiencing menopause-related mental health symptoms access any form of mental health care, compared to 65 percent of white women.2 Psychotherapy use follows a similar pattern: 20 percent versus 36 percent.2 Hispanic women face a 32 percent disparity in menopausal hormone therapy prescriptions, and Black women face a 26 percent gap.3 These numbers point to systemic barriers in both access and provider awareness.
LGBTQ social work practice adds another layer of complexity here. LGBTQ+ individuals experiencing menopause, including trans men and nonbinary people, face compounded challenges. Many encounter provider ignorance about the intersection of hormone therapy and menopausal symptoms, along with stigma that discourages them from seeking care at all. Social workers are often the most accessible point of contact for these populations, making menopause literacy especially consequential in affirming practice settings.
The Misdiagnosis Problem
Menopause-related cognitive and mood symptoms are frequently misattributed to primary mood disorders, adult-onset ADHD, or generalized stress. A client presenting with new concentration difficulties, sleep disruption, and low mood at age 47 may receive an antidepressant or stimulant prescription without anyone asking about cycle changes, hot flashes, or night sweats. This matters for social workers because intake and biopsychosocial assessments set the trajectory for treatment planning. When menopause is not considered as a contributing or primary factor, interventions may target the wrong mechanism, leaving the client undertreated and frustrated.
Social workers who learn to ask about menstrual cycle status, perimenopause symptoms, and reproductive history during routine assessment can catch what other providers miss, improving diagnostic accuracy and ensuring clients receive appropriate, timely care.
Questions to Ask Yourself
Assessment and Screening Tools for Social Workers
Social workers are often the first behavioral health professionals to observe patterns of distress in midlife women, yet standard intake forms rarely probe for menopause-related symptoms. A client presenting with new-onset insomnia, tearfulness, and difficulty concentrating at age 48 may screen as moderately depressed on a PHQ-9 without anyone asking whether her periods have changed or whether hot flashes are disrupting her sleep. Layering menopause-specific screening onto traditional mental health social work assessments allows practitioners to recognize the full context of a client's experience and to differentiate hormone-driven mood changes from primary psychiatric disorders.
Core Mental Health Screens: PHQ-9 and GAD-7
The Patient Health Questionnaire-9 (PHQ-9) and the Generalized Anxiety Disorder-7 (GAD-7) remain foundational tools for any social work assessment. The PHQ-9 consists of nine items that screen for depressive symptom severity, with scores of 5, 10, and 15 marking thresholds for mild, moderate, and moderately severe depression.1 The GAD-7 mirrors this structure with seven items addressing anxiety, using the same cut-points.2 Both instruments are validated for diagnostic screening in general adult populations and carry the advantage of brevity and widespread familiarity among interdisciplinary teams. When a woman in her late 40s or early 50s scores in the moderate range on either scale, the next step is to ask whether menopausal transition might be contributing to or amplifying the symptoms captured by these tools.
Menopause-Specific Instruments
Two validated scales bring menopause itself into the foreground: the Menopause Rating Scale (MRS) and the Greene Climacteric Scale. The MRS comprises 11 items organized into somatic, psychological, and urogenital domains, designed to evaluate menopausal symptom burden and its impact on quality of life.2 The Greene Climacteric Scale expands to 21 items covering psychological, physical, and vasomotor or sexual domains, offering finer granularity for assessing symptom severity across the full spectrum of menopause experience. Both scales are well-accepted in research and clinical settings, and neither requires formal diagnostic authority to administer. A social worker can deploy the MRS or Greene scale as part of an intake or progress-monitoring session, then share the results with the client's primary care or gynecology provider to inform medical workup.
When a client scores high on the psychological subscale of either instrument and also endorses frequent hot flashes or night sweats on the vasomotor items, the pattern suggests menopause-related mood disturbance rather than a stand-alone major depressive episode.4 Conversely, if the psychological score is elevated but vasomotor and somatic scores are low, primary mood or anxiety disorder becomes more likely.
Practical Screening Questions for the Psychosocial Interview
Formal questionnaires are valuable, but social workers also need open-ended language that fits naturally into a conversational intake. Consider weaving in the following prompts:
- "Have your periods changed in pattern, length, or intensity over the past year?"
- "Are you experiencing hot flashes, night sweats, or new sleep problems alongside the mood changes you've described?"
- "Have you noticed that your anxiety or low mood gets worse at certain times in your cycle, or has it become more constant as your cycle has become irregular?"
- "Is there a family history of early menopause, and have you ever had your ovaries removed or received cancer treatment that might have affected your hormones?"
These questions serve two purposes: they normalize menopause as a topic within the therapeutic relationship, and they generate timeline data that helps distinguish menopause-related symptoms (which typically emerge or intensify as cycles become irregular) from longstanding psychiatric conditions.
Differentiating Menopause-Related Mood Changes from Primary Disorders
Timing is the most powerful differentiator. If a client reports no prior history of major depression and her first episode of sustained low mood coincides with menstrual irregularity in her mid-to-late 40s, perimenopause is the more parsimonious explanation. Co-occurrence of vasomotor symptoms strengthens that hypothesis; research shows that women who experience frequent hot flashes and night sweats face significantly higher rates of depressive symptoms during the menopause transition.2 When the Greene Climacteric Scale or MRS reveals high scores in both the vasomotor and psychological domains, the practitioner should document that pattern and recommend hormonal evaluation by a physician.4
Social workers are not diagnosing menopause, nor are they prescribing hormone therapy. The role is to identify patterns, document them systematically, and coordinate with medical providers so that clients receive comprehensive, interdisciplinary care. By pairing the PHQ-9 and GAD-7 with menopause-specific tools and thoughtful open-ended questions, social workers position themselves as essential links between behavioral health and women's health systems.
Screening Tool Quick-Reference
Social workers assessing midlife clients should be familiar with validated instruments that capture both menopausal symptom severity and co-occurring mental health concerns. The tools below can be integrated into intake assessments, ongoing monitoring, or interdisciplinary care coordination. Selecting the right combination allows practitioners to distinguish between primary mood disorders and menopause-related psychological disturbances, which is essential for effective treatment planning.
| Tool | What It Measures | Items / Time to Administer | Best Use in Menopause Context |
|---|---|---|---|
| PHQ-9 (Patient Health Questionnaire-9) | Depression severity across nine DSM criteria | 9 items / approximately 3 to 5 minutes | Tracking depressive symptoms that may emerge or intensify during perimenopause and menopause, including changes in sleep, energy, and concentration |
| GAD-7 (Generalized Anxiety Disorder-7) | Anxiety symptom frequency and severity | 7 items / approximately 3 minutes | Identifying anxiety that often co-occurs with hormonal shifts, distinguishing clinical anxiety from transient menopausal distress |
| Menopause Rating Scale (MRS) | Somatic, psychological, and urogenital symptom severity specific to menopause | 11 items / approximately 5 minutes | Providing a menopause-specific symptom profile that captures the full range of complaints, including mood, sleep disruption, and cognitive changes |
| Pittsburgh Sleep Quality Index (PSQI) | Subjective sleep quality, latency, duration, efficiency, and disturbances | 19 items / approximately 5 to 10 minutes | Evaluating sleep disruption, which affects over 80% of menopausal individuals and contributes directly to depression and cognitive difficulty |
| Greene Climacteric Scale | Psychological, somatic, and vasomotor symptoms during the menopausal transition | 21 items / approximately 5 to 7 minutes | Differentiating psychological symptoms (anxiety, depression) from vasomotor and somatic complaints to guide targeted psychosocial interventions |
| ISI (Insomnia Severity Index) | Perceived insomnia severity, satisfaction with sleep, and daytime impairment | 7 items / approximately 3 minutes | Serving as a brief complement to the PSQI when time is limited, particularly useful for repeated monitoring in clinical social work sessions |
Evidence-Based Psychosocial Interventions
Social workers already possess the clinical training to deliver some of the most effective nonpharmacological treatments for menopausal mental health symptoms, and the research backing those interventions is now substantial.
Cognitive Behavioral Therapy Adapted for Menopause
CBT is the most rigorously studied psychosocial intervention for menopause-related distress, and it falls squarely within the licensed clinical social worker's scope of practice. A 2024 meta-analysis spanning 30 studies and more than 3,500 participants found that CBT produced meaningful reductions in both depressive and anxiety symptoms among menopausal women.1 Depression scores dropped by roughly 55 percent in CBT groups compared with only 15 percent in control conditions. Group-delivered CBT showed particularly strong results for anxiety, with a 50 percent reduction versus 30 percent in individual formats.
The landmark MENOS trials demonstrated that CBT also targets vasomotor symptoms directly, reducing hot-flash frequency by 30 to 50 percent and significantly lowering the distress those episodes cause.2 Quality-of-life gains were among the largest effects observed, with group CBT producing especially robust improvements. Notably, when CBT was combined with hormone replacement therapy, anxiety and depression reductions were greater still (40 percent and 35 percent, respectively), underscoring the value of interdisciplinary collaboration. Social workers who deliver menopause-adapted CBT can position themselves as essential members of that care team.
Psychoeducation Group Models
Structured psychoeducation groups, typically running six to eight sessions, give social workers a scalable way to reach more clients while building community. A well-designed menopause psychoeducation group covers topics such as the biology of hormonal change, sleep hygiene strategies, cognitive restructuring for mood symptoms, body-image shifts, relationship communication, and goal setting for the post-menopausal years. Published programs show that participants report higher self-efficacy around symptom management and meaningful reductions in both psychological distress and perceived symptom severity by the final session. The group format itself appears therapeutic: shared experience normalizes symptoms that many women have been told to simply endure.
Motivational Interviewing and Stress Management
Midlife often brings a cluster of health-behavior challenges, from declining physical activity and disrupted sleep to increased alcohol use as a coping mechanism. Motivational interviewing (MI) is an evidence-based technique social workers are trained to use, and it adapts well to conversations about exercise adoption, sleep-hygiene routines, and substance-use reduction during perimenopause. Pairing MI with mindfulness-based stress reduction (MBSR) strengthens outcomes further. A 2024 review of mindfulness-based interventions for menopausal women found notable reductions in anxiety symptoms, and the approach also showed a positive, though smaller, effect on depressive symptoms.1 An eight-week MBSR curriculum can be co-facilitated by social workers alongside other behavioral health providers, giving clients concrete tools for managing the heightened stress reactivity common during the menopausal transition.
Community-Based and Peer Support Models
Social workers are uniquely positioned to create and lead community-level supports that extend well beyond the therapy office. Peer support groups and menopause cafes, informal gatherings where women discuss symptoms and coping strategies over coffee, have gained traction internationally as low-barrier entry points to care. Online counseling and virtual support communities expand reach even further, particularly for women in rural areas or those whose work schedules make in-person attendance difficult. While large-scale controlled trials on these formats remain limited, preliminary outcome data indicate that regular participation is associated with reduced feelings of isolation, increased health-information seeking, and greater willingness to pursue clinical treatment. Social workers who facilitate these groups can also use them as screening opportunities, identifying participants whose symptom severity warrants a referral for CBT, medication evaluation, or both.
Taken together, these interventions give social workers a versatile, evidence-backed toolkit for addressing menopause-related mental health concerns across settings, from private practice and hospital-based women's health clinics to community centers and telehealth platforms. Social work research and practice from institutions such as the Massachusetts General Hospital Center for Women's Mental Health continues to refine best practices, reinforcing that psychosocial care is not a secondary add-on but a frontline treatment for menopausal distress.2
Related Articles
Addressing Workplace Impacts and the Social Worker's Advocacy Role
Menopause symptoms do not stop when a woman clocks in for work. Cognitive fog, sudden fatigue, temperature sensitivity, and concentration lapses frequently collide with professional demands, yet stigma pushes many to suffer in silence rather than request support. Social workers in employee assistance programs and HR settings are positioned to dismantle that silence through education, policy change, and direct advocacy for reasonable accommodations.
When Menopause Enters the Workplace
Productivity can erode when hot flashes interrupt focus or sleep disruption feeds daytime exhaustion. Research consistently shows higher absenteeism and presenteeism among midlife women, but the reason is rarely openly discussed. Many employees fear that disclosing menopause will damage their credibility or invite ageist and sexist assumptions. Social workers bring a clinical lens to this dynamic, recognizing that untreated symptoms often amplify anxiety and depression, creating a cycle that affects both health and career trajectory.
The Social Worker as Policy Advocate and Educator
Within EAPs and human resources, social workers lead initiatives that normalize menopause as a workplace health topic. Concrete actions include drafting menopause-friendly policy templates that offer flexible scheduling, access to temperature-controlled breakout spaces, and modified break allowances. A social worker might train managers to recognize how cognitive symptoms present and to respond without judgment when an employee seeks adjustments. Employer education can be formalized through lunch-and-learn sessions or annual wellness campaigns, framing menopause awareness as a retention and inclusion issue. These efforts connect naturally to broader conversations about women in social work leadership and how the profession itself models gender-responsive institutional culture.
Navigating ADA and Reasonable Accommodations
Menopause itself is not a disability under the Americans with Disabilities Act, but its severe psychiatric sequelae can be. Major depression, incapacitating anxiety, and sleep disorders linked to perimenopause may meet the threshold for protection. Disability social workers bring specific expertise to this area, guiding clients through the accommodation process, documenting functional limitations, and connecting symptoms to specific workplace barriers. They help craft requests like modified duties during acute episodes, environmental controls, or leave adjustments, ensuring the process is collaborative rather than adversarial.
Championing Menopause as a DEI Priority
Forward-thinking social workers treat menopause accommodation as a diversity, equity, and inclusion issue. They collect anonymous workplace climate data, develop policy templates that other organizations can adopt, and build coalitions with women's health advocates. By tying these efforts to broader DEI goals, they shift menopause from a private embarrassment to a systematic concern that the institution is responsible for addressing.
Menopause-related productivity loss and turnover cost employers billions each year, yet fewer than 10 percent of workplaces maintain any menopause policy. Social workers in employee assistance programs and occupational health settings can lead policy development, accommodation protocols, and supervisor training, directly reducing attrition and improving workplace mental health for millions of midlife women.
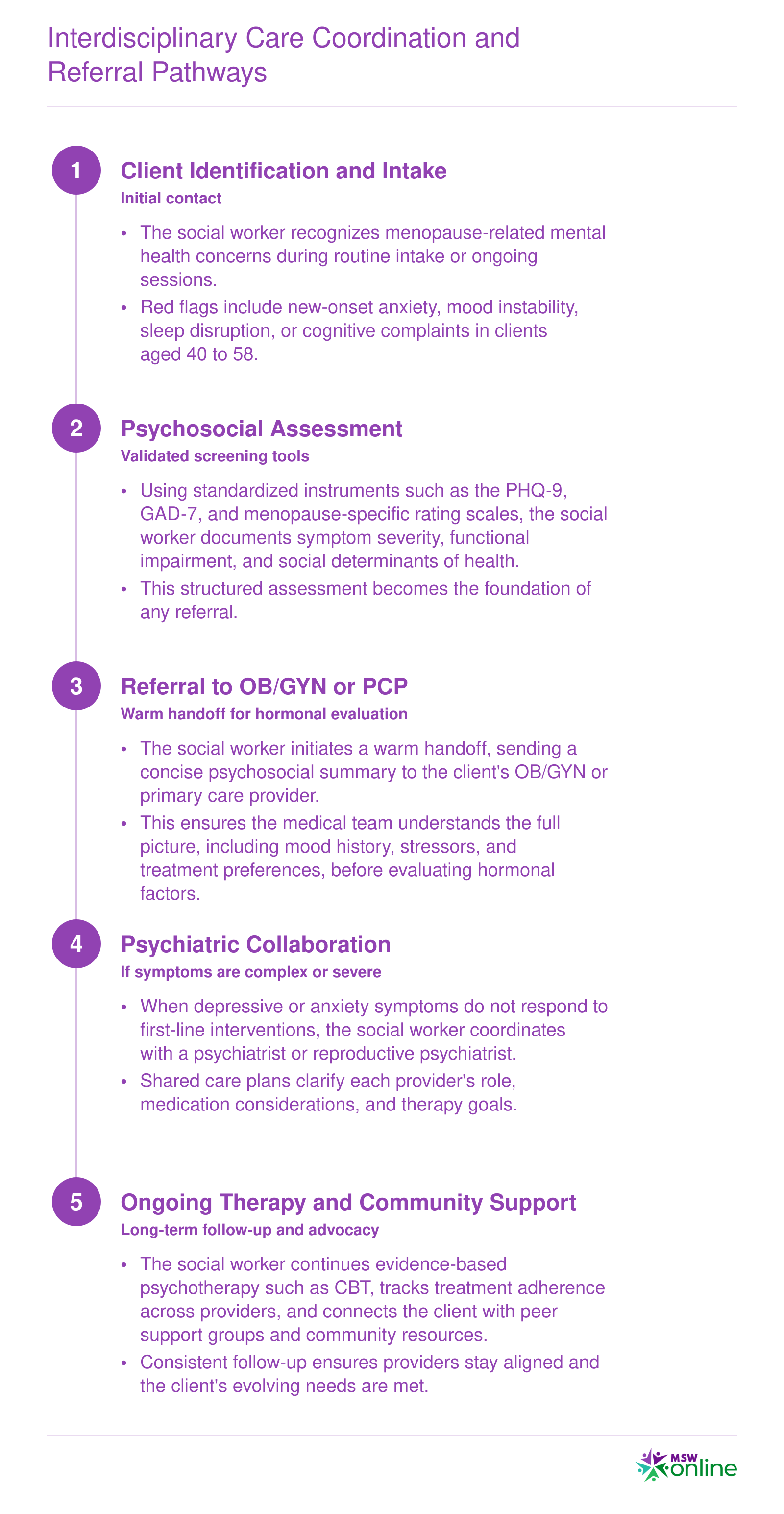
Interdisciplinary Care Coordination and Referral Pathways
Social workers serve as the central hub in midlife mental health care, bridging communication gaps between gynecologists, primary care providers, psychiatrists, and psychologists. By translating a client's psychosocial context for medical teams, coordinating warm handoffs, maintaining shared care plans, and tracking follow-up, social workers ensure that menopause symptoms are neither dismissed nor treated in isolation. This coordination sequence outlines the practical workflow from first contact through ongoing support.
The Menopause Behavioral Health Certification (MBH-C): A New Career Credential
A new credential can cost a professional time and money with no guarantee of return. The MBH-C is worth evaluating carefully, because the gap it fills is real and the career timing is early enough to matter.
What FamilyWell Health Launched
On June 18, 2026, FamilyWell Health launched The Menopause Hub, a dedicated platform for menopause-focused behavioral health training and resources.1 The centerpiece for social workers is the Menopause Behavioral Health Certification (MBH-C), described as the first accredited interprofessional continuing education credential in menopause behavioral health. Accreditation runs through joint providership with Innovation Horizons under an Interprofessional Continuing Education (IPCE) framework, which means the credits are recognized across disciplines, with profession-specific credit available for social workers, psychologists, nurses, dietitians, coaches, and community health workers, among others.2
Nearly 400 providers had already joined the waitlist before the certification formally opened for enrollment, a signal that demand in this niche is not hypothetical.1
Program Structure and Cost
The MBH-C is delivered entirely online, built around 15 self-paced modules supplemented by live mentorship sessions. The full program awards 23 continuing education credits, and enrollment is available through the Menopause Hub waitlist at a program cost of $999.3 CE credit availability began June 15, 2026, putting the certification in its opening weeks as of this writing.
For social workers who track continuing education requirements carefully, the IPCE structure is practical. Credits apply toward licensure renewal in most states that accept interprofessional CE, though individual practitioners should confirm with their state licensing board. Social workers who want context on how specialty certifications function within trauma certification for social workers programs can benchmark the MBH-C against that established model.
The Free White Paper: An Immediate Starting Point
Alongside the certification, FamilyWell Health released a free clinical white paper written by Dr. Jessica Gaulton (founder and CEO), Dr. Marissa Caan (Medical Director and reproductive psychiatrist), and Dr. Melissa Sherman (OB/GYN physician and medical advisor).1 For social workers who are not yet ready to commit to the full certification, the white paper offers evidence-based guidelines on recognizing and managing mood disorders during perimenopause and menopause at no cost. It is a practical first step before pursuing the credential.
What Comes Next for Interdisciplinary Teams
FamilyWell Health has announced a companion credential, the Menopause Behavioral Health Physician Certificate (MBH-PC), planned for fall 2026.2 The MBH-PC is CME-accredited and aimed at OB/GYNs, primary care physicians, family medicine physicians, and nurse practitioners. For social workers already holding the MBH-C, a physician or NP colleague earning the MBH-PC creates a shared clinical language across the care team, which strengthens referral pathways and collaborative care.
Why Early Certification Creates Career Leverage
Menopause care is consolidating into a recognized subspecialty faster than training infrastructure has kept pace. Women's health clinics, employee assistance programs, telehealth platforms, and community health centers are beginning to build midlife care programs, and most lack staff with any formal menopause behavioral health training. The social work role in healthcare literature consistently shows that early specialization improves both patient outcomes and practitioner positioning. An MSW who holds the MBH-C in 2026 enters that landscape ahead of the credentialing curve rather than catching up to it. Specialty does not always require a new degree; sometimes it requires being first in a defined space.
Career Outlook and Salary for Social Workers in Midlife Care
The two occupation categories most relevant to menopause-focused social work are Healthcare Social Workers and Mental Health and Substance Abuse Social Workers. Both fields are growing significantly faster than the national average for all occupations (roughly 4 percent over the 2023 to 2033 decade), reflecting rising demand in integrated behavioral health, women's health programs, and telehealth platforms. The salary figures below come from 2024 Bureau of Labor Statistics Occupational Employment and Wage Statistics data and should be treated as approximate benchmarks. Because social work degree programs map to multiple occupation codes, individual earnings will vary by setting, geography, and specialization. Emerging career pathways for social workers with menopause and midlife expertise include women's health positions in hospital systems, integrated behavioral health clinics that co-locate mental health providers alongside OB/GYNs, telehealth menopause care platforms such as FamilyWell Health, and Employee Assistance Programs that address midlife workplace challenges. Credentials like the Menopause Behavioral Health Certification (MBH-C) may strengthen candidacy for these roles by signaling specialized, evidence-based training that employers and interdisciplinary teams increasingly value.
| Occupation | Total National Employment | 25th Percentile Salary | Median Salary | 75th Percentile Salary | Mean Salary | Projected Job Growth |
|---|---|---|---|---|---|---|
| Healthcare Social Workers | 185,940 | $55,360 | $68,090 | $83,410 | $72,030 | 10% (2022 to 2032) |
| Mental Health and Substance Abuse Social Workers | 125,910 | $46,550 | $60,060 | $78,980 | $68,290 | 11% (2023 to 2033) |
| All Social Workers | 759,740 | $48,680 | $61,330 | $78,500 | $67,050 | 6% (2024 to 2034) |
Frequently Asked Questions About Menopause and Social Work
The intersection of menopause and social work practice raises important questions for clinicians, advocates, and professionals considering this emerging specialty. Below are answers to the most common questions, with references to relevant sections of this guide for deeper exploration.
Menopause is an underserved psychosocial issue, and social workers are better positioned than almost any other profession to address it. Person-in-environment training, clinical assessment skills, and comfort navigating stigma-laden conversations are exactly what midlife clients need but rarely receive from a single provider.
The practical path forward is clear: add a validated screening tool to your intake process, review the free clinical white paper from FamilyWell Health, and consider pursuing the MBH-C certification before the field becomes crowded. Mental health social workers who specialize in midlife care now will not be catching up to this field as employers build menopause policies and interdisciplinary teams seek behavioral health leads. They will be defining it.