Points of interest…
- J, a 20-year-old with autism, waited 121 hours in a psych ER after his mother left him at triage.
- Psychiatric ER social workers in dedicated units manage 8-15 patients, while general ED consults can exceed 25.
- Healthcare social workers earned a median $68,090 in 2024, with mental health social workers at $60,060.
- Compassion fatigue strikes most psychiatric social workers, underscoring the emotional toll of constant crisis exposure.
Psychiatric emergency rooms have become the nation’s de facto crisis safety net, absorbing a surge in mental health visits that the outpatient system cannot handle. Social workers hold that front line, bridging acute clinical needs and shattered community supports.
In a single shift, a psychiatric ER social worker may de-escalate a violent behavioral crisis and then spend hours hunting for a residential placement that doesn’t exist, often for patients like J, a 20-year-old with autism whose mother left him at triage after he punched her. The work exacts an emotional toll that directly influences career trajectory and earning power.
What Does a Psychiatric ER Social Worker Do? A Shift Breakdown
What does a psychiatric ER social worker actually do during a 12-hour shift1? The role blends crisis triage, rapid assessment, and real-time resource navigation, often with little warning about what the next hour will bring. In a dedicated psychiatric emergency service (PES), the workflow is more focused than a general emergency department, but the intensity is constant.
The First Hours: Huddle and Triage
A shift often starts with a team huddle alongside the psychiatrist, nurse practitioner, and nursing staff2 to review overnight holdovers and anticipated arrivals. Then the real pace begins. As patients arrive, the social worker performs a 10- to 20-minute triage assessment3, gathering the immediate reason for the visit, any known psychiatric history, and current risk factors. In this compressed window, the social worker screens for suicide risk by probing intent, plan, means, protective factors, and any history of attempts or violence3. The goal is not a full psychosocial exploration but a quick determination: can this person wait safely, or do they need immediate intervention?
Mid-Shift: Crisis Intervention and Assessment
Once triaged, patients needing a deeper look receive a full psychosocial assessment4. The social worker coordinates with nursing and security for de-escalation if a patient becomes agitated, a key component of social worker safety in mental health settings, validating distress, clarifying the immediate crisis, and identifying short-term coping strategies3. For complex cases, family meetings become essential: providing psychoeducation on illness and crisis response, especially for adolescents or first-episode psychosis2. Throughout the shift, the social worker balances constant triage of new arrivals against documentation of these assessments in the electronic medical record3. Supportive counseling helps patients tolerate the prolonged ED stay while awaiting a bed or family3.
Afternoon Rounds: Disposition and Discharge Planning
Mid-afternoon, the team reconvenes for disposition rounds. The social worker presents each case: will the patient be admitted, transferred to a crisis residential bed, or discharged with intensive outpatient follow-up?1 When admission is necessary, the social worker sends clinical summaries and makes calls to behavioral health units to secure a bed5. For voluntary admissions, they obtain signatures; for involuntary holds, they document the legal status3. Discharge plans are built around follow-up appointments, safety plans, and clear return instructions2. Disposition decisions feel weightier here than in standard case management because of the acute danger and unpredictable volume, resources must be brokered in hours, not weeks.
End of Shift: Wrap-Up and Handoff
Before leaving, the social worker completes mandated reports to child or adult protective services if needed4, finalizes transfer packets (psychosocial assessment, risk assessment, medication list, legal documents)1, and briefs the oncoming shift. Unlike a traditional clinical case manager who carries a stable caseload, the psychiatric ER social worker has been in constant prioritization mode, answering a relentless series of emergent needs with limited background information and high stakes.
Inside the Psychiatric ER: A Night in the Life
A 121-Hour Wait for a Home That Never Came
In a crowded psychiatric emergency room, a 20-year-old named J sat in an extended observation room. He has an intellectual disability and autism spectrum disorder. His mother brought him to the hospital after he punched her during a behavioral crisis. Overwhelmed and without support, she left him at triage and did not return. For 121 hours, J remained in the ER, caught in a holding pattern with no clinical need for psychiatric hospitalization and no safe discharge destination.1 A psychiatry resident, Ashley Andreou, described ordering intramuscular Thorazine to sedate him during an outburst, not because he had psychosis, but because the environment itself was causing distress.
The Crumbling Safety Net: When Respite Care Is Absent
J’s story is not unique. Families caring for loved ones with developmental disabilities often reach a breaking point when community-based supports fail to materialize. Respite care, crisis beds, and in-home behavioral services are chronically underfunded and understaffed. When these resources are missing, the psychiatric ER becomes the default safety net. This systemic gap forces emergency services to warehouse people who need social support, not psychiatric treatment.
The Social Worker as Advocate: Seeking Non-Clinical Solutions
For the psychiatric social worker, J’s case is a call to action. The clinical team can manage immediate agitation, but the real solution lies outside the hospital walls. Social workers in these settings must be relentless advocates, pushing for referrals to developmental disability agencies, applying for residential placements, and coordinating with state-funded respite programs. They assess for safety, coordinate with mobile crisis teams, and document the lack of appropriate placements to drive systemic change. They often work against a tide of bureaucracy, but their interventions can prevent repeat ER visits and reduce caregiver burnout.
Medical Interventions Are Only a Bandage
Andreou’s use of Thorazine highlights a stark reality: when social supports collapse, medical providers are left to manage social crises with sedatives and safety holds. Extended observation units with constant monitoring become temporary shelters. A technician was scratched by J during a behavioral episode, an incident common when staff become de facto caregivers for individuals with complex needs. The psychiatric ER social worker bridges this gap, translating medical despair into tangible community connections that address the root causes of crisis.
Related Articles
Questions to Ask Yourself
Crisis Intervention and De-Escalation: Tools and Tactics
Effective crisis intervention in a psychiatric emergency room is not about overpowering a patient; it’s about out-communicating a crisis. Social workers use a layered approach that starts with verbal techniques, progresses to structured risk assessment, and, only when all else fails, turns to pharmacological intervention as a last resort.
Verbal De-escalation and Environmental Safety
Verbal de-escalation relies on a foundation of active listening, empathetic validation, and clear boundary setting. Clinicians maintain a recommended distance of at least two arm’s lengths1 to preserve personal safety while projecting calm. The three-step model, often summarized as assess, engage, and resolve, guides workers to first evaluate the immediate threat, then connect with the patient’s experience, and finally establish mutual limits.2 Tools like the STAMP Observation Tool help staff catch early signs of agitation before they escalate. STAMP stands for Staring, Tone, Anxiety, Mumbling, and Pacing, five behavioral cues that appear on a continuum and allow for early redirection.3 Environmental safety measures, such as removing potential weapons and ensuring escape routes, run in parallel with these conversations.
Risk Assessment with Standardized Tools
Once the immediate emotional temperature is lowered, social workers turn to standardized instruments to quantify risk. The Columbia-Suicide Severity Rating Scale (C-SSRS) provides a structured flowchart of questions that assesses recent suicidal ideation, plan, and intent. For a broader snapshot of a patient’s psychiatric state, the Brief Psychiatric Rating Scale (BPRS) measures symptoms like hostility, suspiciousness, and emotional withdrawal, creating a baseline that guides intervention. The Behavioral Activity Rating Scale (BARS), a seven-point scale3 ranging from difficult to arouse to out of control, adds yet another layer, ensuring that agitation is documented objectively. These tools do not replace clinical judgment but anchor it in evidence, helping to justify the next steps, including, when necessary, the decision to use medication.
When Words Aren’t Enough: Chemical Sedation and Ethical Boundaries
Despite the best verbal efforts, some crises demand chemical sedation to prevent harm. The goal of sedation is calm, not heavy sedation,2 and common combinations like haloperidol plus a benzodiazepine4 are chosen for rapid effect. The ethical tension for social workers is acute: medications like Thorazine, when used for behavioral control rather than treating an underlying illness, can feel like a betrayal of the patient-centered values the profession upholds. Four principles of crisis intervention ethics, respect for autonomy, beneficence, nonmaleficence, and justice, must be weighed in seconds.1 The social worker’s role is to advocate for the least restrictive measure, document the clear failure of verbal techniques, and ensure that the patient’s voice is still heard.
The Interdisciplinary Response
No single discipline manages a behavioral crisis alone. A coordinated team response involving at least six disciplines: psychiatry, nursing, social work, security, behavioral health technicians, and sometimes pharmacy, executes a choreographed intervention.1 The psychiatrist orders the medication, the nurse administers it, and the social worker maintains therapeutic engagement throughout, providing verbal reassurance and monitoring for side effects. The social worker also bridges communication with family, documents the event from a psychosocial perspective, and debriefs the team afterward. This interdependence prevents any one professional from carrying the full emotional weight and ensures that safety and dignity are balanced across every decision.
Navigating Involuntary Holds: The Social Worker’s Legal and Ethical Role
Involuntary psychiatric holds are among the most legally charged actions a social worker can undertake in an emergency setting, requiring immediate clarity on state-specific criteria and unwavering adherence to ethical practice. Social workers must know exactly when a hold is justified, how to document it, and how to balance client autonomy with imminent safety risks. The following resources and steps can guide you through this complex terrain.
Understanding State-Specific Involuntary Hold Laws
Every state defines its own threshold for involuntary commitment, often using terms like "danger to self or others" or "gravely disabled." Social workers should:
- Review your state's mental health code: Statutes typically outline the duration of holds (e.g., 72-hour observation), criteria for extension, and who may initiate them. Many state health department websites publish plain-language summaries.
- Identify the key legal pathways: Some states allow social workers to directly place a hold; others require a peace officer or physician signature. Know your scope and the chain of authority.
- Stay current with legislative updates: Laws can change, especially in response to high-profile cases. Set alerts for your state legislature’s health committee.
Ethical Guidelines and Practice Standards
Beyond the statute, social work ethics demand a person-centered approach. The National Association of Social Workers (NASW) provides state chapters that often issue practice alerts on involuntary care. Actionable steps include:
- Consult your state’s NASW chapter: Many chapters publish guidance on balancing safety with the least restrictive alternative. They may also offer ethics consultations for difficult cases.
- Apply the social work code of ethics: Core values like self-determination and dignity must be weighed against the duty to protect. Always document your reasoning, including why less restrictive measures were insufficient.
- Seek supervision and peer review: Ethical dilemmas often benefit from multidisciplinary ethics committees or social work supervisors who can help untangle conflicting obligations.
Documentation and Capacity Evaluations
Initiating a hold requires meticulous legwork. Social workers typically:
- Assess decision-making capacity: Capacity is situation-specific; a person may be able to refuse medication but not understand the risk of leaving. Use standardized tools if your facility provides them, but always supplement with clinical judgment.
- Write a thorough affidavit or petition: Detail observable behaviors, direct statements, and collateral information. Avoid jargon; courts need a clear narrative of why the person meets the legal standard.
- Include risk and protective factors: Note any family support, housing instability, or treatment history that contextualizes the crisis. This demonstrates a holistic assessment rather than a punitive stance.
Local Procedures and Training Resources
Finally, practical wisdom lives within your own community. To build competence:
- Contact your local community mental health center: These agencies often coordinate the inpatient placement process and can brief you on county-specific forms, timelines, and emergency contacts.
- Tap into hospital social work departments: If you work in a psychiatric emergency room, your own department likely maintains an internal resource guide with phone numbers for judges, crisis teams, and local advocacy organizations.
- Pursue targeted continuing education: Many state licensing boards approve courses on involuntary treatment law, trauma-informed de-escalation, and documentation. Check your board’s website for upcoming offerings or recommendations.
J's mother left him at triage and has not taken him home for 121 hours.
Compassion Fatigue and Burnout: The Emotional Cost of Crisis Work
Frontline psychiatric social workers are confronting a silent epidemic of emotional exhaustion, with studies now showing that most will experience compassion fatigue at some point in their careers. The constant exposure to trauma, the pressure of split-second crisis decisions, and the moral weight of working within a fractured system take a measurable toll.
The Distinct Burdens: Compassion Fatigue, Secondary Trauma, and Burnout
These terms are often used interchangeably, but they describe related yet distinct experiences. Compassion fatigue is the cumulative physical, emotional, and psychological depletion that comes from caring for others in distress. It encompasses secondary traumatic stress, which mirrors symptoms of post-traumatic stress disorder and arises from indirect exposure to clients' trauma. Burnout, by contrast, develops over time from workplace conditions: chronic emotional exhaustion, a sense of reduced personal accomplishment, and depersonalization, a cynical detachment from the people you serve. A psychiatric ER social worker can experience all three simultaneously, often with one feeding the others.
The Numbers: How Widespread Is the Emotional Toll?
The data paint a stark picture. Research on psychiatric workers nationally indicates that compassion fatigue affects between 67 and 85 percent of those in frontline roles.1 Among social workers, 70.3 percent report high levels of emotional exhaustion, and when moderate cases are included, the figure climbs to 85 percent. Depersonalization is high for 48.5 percent. Lifetime burnout rates for social workers reach 75 percent, and 62 percent experienced burnout within the past year alone.1 One survey from 2024 found that more than half of social workers scored at a medium or higher level for compassion fatigue.2 Specific subgroups fare even worse: child welfare social workers, for instance, register at the 94th percentile for secondary traumatic stress.2 Among social workers and case managers, 56 percent report compassion fatigue symptoms, and 49 percent describe emotional numbness.3
The Weight of Systemic Failures: Cases Like J's
These statistics are not abstractions. In the STAT News piece, a psychiatric resident describes a young man with autism and intellectual disability who remained in the ER for 121 hours after his mother, overwhelmed and without adequate community supports, left him at triage.4 For the social worker involved, such a case is not simply a clinical challenge; it is a window into systemic neglect. When residential placements are scarce, respite care is inaccessible, and families bear impossible burdens alone, the emergency room becomes a default holding pen. Social workers absorb the emotional overflow: the grief of parents, the distress of patients who do not belong in a psychiatric setting, and the frustration of advocating for resources that never materialize. Over time, the accumulation of these impossible situations erodes empathy and fuels moral distress.
Building Resilience: Individual and Organizational Strategies
Addressing the emotional cost of crisis work requires both personal habits and structural change. On an individual level, evidence points to the value of reflective supervision, where practitioners can process cases with a trusted mentor, not just review clinical tasks. Mindfulness-based stress reduction programs have been shown to lower burnout scores and improve emotional regulation. Peer support groups, whether formal or informal, provide a space to normalize the intense reactions this work evokes.
However, resilience cannot rest solely on the shoulders of individual clinicians. Agencies have a responsibility to create trauma-informed workplaces. That means realistic caseloads, mandatory debriefing protocols after critical incidents, and a leadership culture that acknowledges the psychological risks of the job. When organizations treat staff well-being as an afterthought, even the most dedicated social workers will eventually run dry. The most effective interventions combine personal coping skills with an environment that actively prevents chronic overload.
What Do Psychiatric ER Social Workers Earn?
According to the U.S. Bureau of Labor Statistics, healthcare social workers earned a median annual wage of $68,090 in May 2024.
Building the Interdisciplinary Team: Social Workers Out of Silos
Who's Who in the Psychiatric ER
In a crisis, roles must be crystal clear. The attending psychiatrist leads diagnostic formulation and medication decisions, while the psychiatric nurse handles continuous monitoring, medication administration, and safety checks. The social worker takes charge of the psychosocial assessment, disposition coordination, and case management, connecting the dots between the hospital, family, and community resources. Peer recovery specialists offer lived-experience support, and security ensures physical safety. Knowing who does what prevents duplication and gaps, especially when a patient like J arrives after 121 hours in an observation room and needs advocacy that spans clinical and social domains.2
The Crisis Intervention Team (CIT) Model
Many psychiatric ERs partner with law enforcement through CIT programs. Officers receive specialized training in de-escalation and mental health recognition, often through joint simulation exercises with hospital staff. When police bring in a person in crisis, the social worker steps in to coordinate follow-up care and diversion from the ER whenever possible. This model shifts the response from criminalization to treatment. Formal interagency agreements (MOUs) between hospitals, mental health centers, and law enforcement codify these roles, ensuring a seamless handoff and reducing unnecessary psychiatric holds.3
Connecting to Mobile Crisis and Community Supports
Social workers are the linchpin for mobile crisis integration. When a 988 call or a family crisis does not require an ED visit, a community mobile crisis team can stabilize the person at home. The social worker bridges the gap, linking patients to these responders and coordinating with primary care, schools, and housing services. Research shows that coordinated care models can reduce behavioral health ED visits by 25% and hospital admissions by 58%1, outcomes that underscore the value of keeping people out of the hospital when community support suffices. This integration prevents caregiver burnout and inappropriate psychiatric hospitalizations.
Communication and Documentation Practices
Effective teams use daily interdisciplinary huddles to share updates, flag at-risk patients, and align on treatment goals.2 After a critical incident, like a staff scratch or a sedation event, brief debriefs help the team process and adjust protocols. Real-time documentation that flows across disciplines, from nursing notes to social work assessments, ensures everyone works from the same information. A shared language, free of jargon siloes, strengthens the chain of care and protects both patients and providers.
Psychiatric ER Vs. General ED: How the Social Work Role Changes
In a dedicated Psychiatric Emergency Service (PES), a social worker typically carries a caseload of 8 to 15 patients at a time, whereas a social worker covering psychiatric consults in a general emergency department (ED) may handle 10 to 25 consults per shift.1 The numbers themselves reveal how the two environments shape the social work role differently. Where you work profoundly affects how you work.
Environment and Pace
The physical setting of a PES is designed for behavioral health: it is a controlled, lower-stimulus space with observation rooms and on-site psychiatric providers. Patients in a PES stay an average of 12 to 24 hours, and the social work team, which usually numbers 1 to 3 per shift, can focus exclusively on psychiatric crises.1 In contrast, a general ED is a medical-first environment. Psychiatric patients pass through the same chaotic, mixed-acuity bay as stroke and trauma patients, often waiting 12 to 48 hours for a psychiatric evaluation.1 In that setting, a single social worker may be the only behavioral health specialist on shift, pulled from consult to consult without dedicated crisis space.
Role Centrality and Therapeutic Time
Because a PES is a psychiatry-led behavioral health team, the social worker is not an afterthought: the role is central to psychiatric decision making. Social workers in a PES often lead or co-lead discharge planning, and the length of stay affords time for therapeutic engagement, collateral calls, and thorough placement coordination. In a general ED, the social work role is consultative: you are called in by a medically led team, typically for a rapid assessment, a brief intervention, and a handoff back to the medical flow. Contacts are shorter, turnover is faster, and the scope to develop a fuller psychosocial picture is compressed.
Resource Disparities
Resource gaps between the two settings are stark. A PES is far more likely to have dedicated crisis counselors, seclusion-capable observation rooms, and direct relationships with state hospitals and community crisis beds. The presence of an on-site psychiatrist (as opposed to a consult-only psychiatrist in a general ED) means social workers can make real-time clinical decisions and avoid prolonged boarding. In a general ED, you rarely have these built-in connections. Crisis intervention often happens in a hallway or a repurposed exam room, and calls to inpatient programs compete with the overhead of a bustling emergency room.
Involuntary Holds: Same Law, Different Safety
The legal procedure for an involuntary hold is identical no matter which door the patient walks through; the infrastructure to implement it safely differs greatly. In a PES, the controlled environment, constant monitoring, and presence of psychiatric nurses and techs create a safer container for an agitated patient awaiting transfer. In a general ED, the same hold order may unfold in a corner of a busy, understaffed medical floor, where security is stretched thin and staff lack specialized training. For the social worker, this means that your clinical assessment carries the same weight, but your ability to safeguard a vulnerable patient or a distressed family varies with the building you are standing in.
Questions to Ask Yourself
How to Become a Psychiatric ER Social Worker: Education, Licensure, and Career Paths
What degree and license do you need to be hired as a social worker in a psychiatric emergency room? The path is clearly defined, but it demands advanced education, supervised clinical experience, and a commitment to crisis care.
The Foundation: A CSWE-Accredited MSW
A Master of Social Work (MSW) from a program accredited by the Council on Social Work Education (CSWE) is the non-negotiable entry credential for psychiatric social work in crisis settings. This degree provides the core clinical and assessment skills needed to function in a high-acuity environment. Field placements during the MSW are where you build specific expertise. Prioritize internships in inpatient psychiatric units, mobile crisis teams, emergency departments, or dedicated psychiatric emergency services. These settings expose you to rapid triage, risk assessment, and interdisciplinary teamwork under supervision.
The Licensure Ladder: LMSW to LCSW
After earning an MSW, you must obtain a state license to practice. The process typically moves through two stages. First, you earn the Licensed Master Social Worker (LMSW) credential by passing the ASWB Master’s exam. The LMSW allows you to begin working under supervision. To become a Licensed Clinical Social Worker (LCSW) , the standard for independent clinical practice , you must complete a period of supervised clinical work post-master’s. The requirement is usually 3,000 hours or more, accumulated over two to three years, with at least half of those hours in face-to-face psychotherapy or clinical intervention. Then you pass the ASWB Clinical exam. Many psychiatric ER roles require the LCSW, or expect that you will obtain it within a set timeframe.
Credentials That Signal Crisis Expertise
While not required, certifications can sharpen your skills and strengthen your resume. Earning one of the top trauma certifications for social workers, such as the Certified Clinical Trauma Professional (CCTP), shows advanced competency in trauma-informed care, which is central to psychiatric crisis work. The National Association of Social Workers (NASW) offers a clinical social work in psychiatric settings specialty certification for those with substantial post-LCSW experience. Both signal to employers that you understand severe mental illness, de-escalation techniques, and systems-level advocacy.
Where the Career Can Lead
Starting as a frontline clinician, you can advance into roles such as team lead, clinical supervisor, or program manager for psychiatric emergency services. With enough leadership experience and perhaps a management certification, a director-level position overseeing an entire department’s crisis social work becomes attainable. The trajectory rewards those who combine clinical depth with organizational skill.
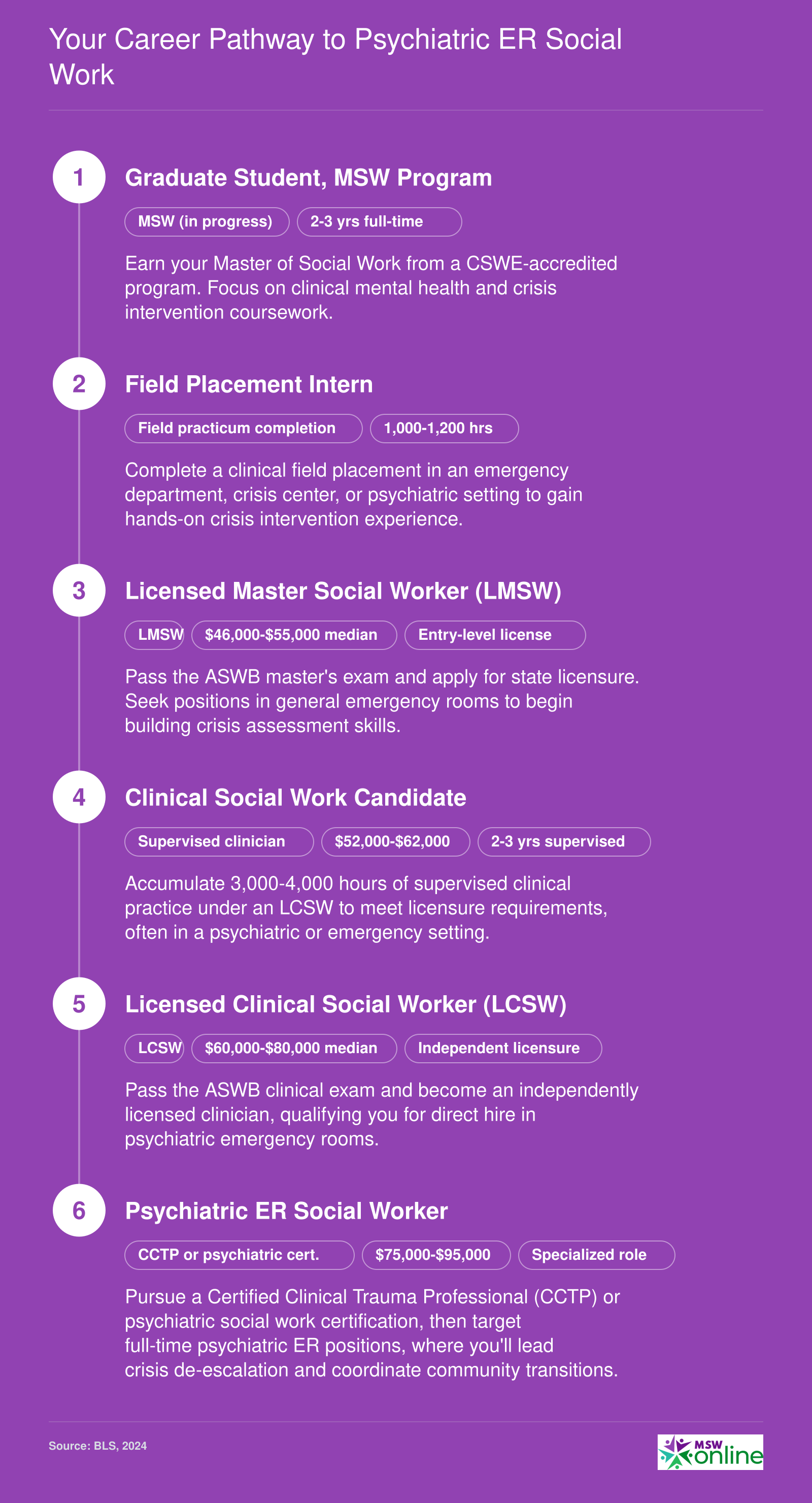
Your Career Pathway to Psychiatric ER Social Work
Social work in psychiatric emergency rooms demands advanced clinical licensure and crisis expertise. This six-step ladder maps the credentials, supervised experience, and salary progression needed to reach this high-impact specialty.
Salary and Job Outlook: Is Psychiatric ER Social Work a Growing Field?
Bureau of Labor Statistics data show that mental health and substance abuse social workers earn a national median of $60,060, while healthcare social workers earn $68,090. Both occupations are projected to grow much faster than the average for all occupations through 2034, at 9.7% and 10% respectively, adding tens of thousands of new positions. For psychiatric ER social workers, actual earnings can be higher: many hospitals offer night and weekend shift differentials, on-call stipends, and competitive pay to retain staff in these high-stress, round-the-clock environments.
| Occupation | Total Employment (2024) | Median Annual Wage | 25th Percentile | 75th Percentile | Projected Job Growth (2024-2034) |
|---|---|---|---|---|---|
| Mental Health and Substance Abuse Social Workers | 125,910 | $60,060 | $46,550 | $78,980 | 9.7% (13,300 new jobs) |
| Healthcare Social Workers | 185,940 | $68,090 | $55,360 | $83,410 | 10% (26,300 new jobs) |
| Social Workers (Overall) | 759,740 | $61,330 | $48,680 | $78,500 | 6% |