Points of interest…
- An estimated 62% of social workers reported burnout in the past year, with child welfare showing the highest rates.
- New Brunswick exit rates doubled from roughly 5% before 2019 to about 10% afterward, signaling a systemic retention crisis.
- The Maslach Burnout Inventory remains the gold-standard assessment tool, yet most social workers have never completed one.
- Written, monthly-reviewed burnout prevention plans outperform mental checklists for sustaining long-term self-care habits.
Social work's turnover problem is getting worse, not stabilizing. Before 2019, annual exits from social work practice in New Brunswick ran between 5 and 6 percent. After 2019, that figure jumped to roughly 10 percent, a near-doubling documented by a DataNB workforce study tracking registered social workers from 2010 to 2024.1 That pattern almost certainly extends beyond one Canadian province.
The profession is adding practitioners, but it is losing frontline workers at an accelerating rate. Caseload pressure, compensation gaps, and organizational cultures that treat self-care as a personal responsibility rather than a structural commitment are driving people out. Those who stay carry heavier loads as a result.
Understanding burnout means distinguishing it from compassion fatigue and vicarious trauma, identifying it early with validated tools, and matching interventions to your career stage. The workforce data makes clear that this is a systemic problem requiring systemic responses, not just individual coping strategies for MSW students and early-career practitioners.
What Is Social Worker Burnout, and How Is It Different From Compassion Fatigue?
The terms burnout, compassion fatigue, and vicarious trauma are used interchangeably in many social work settings, but the distinctions are critical for choosing effective interventions. A social worker who is emotionally exhausted from administrative overload needs different support than one who has absorbed the trauma of a child welfare caseload.
Burnout: Chronic Workplace Stress
Burnout, as defined by Christina Maslach's widely adopted framework, is a syndrome resulting from chronic workplace stress that has not been successfully managed. It manifests in three dimensions: emotional exhaustion (feeling depleted and unable to recover), depersonalization (cynicism or detachment from clients and colleagues), and reduced personal accomplishment (a sense that your work no longer makes a difference). Burnout is primarily a response to organizational and structural conditions, such as high caseloads, inadequate supervision, role ambiguity, and lack of control over decision-making. It can occur in any helping profession, but social workers face elevated risk because of systemic underfunding, administrative burden, and the emotional labor inherent in direct practice.
Compassion Fatigue and Vicarious Trauma: Secondary Exposure to Trauma
Compassion fatigue refers to the emotional and physical exhaustion that arises from absorbing clients' traumatic experiences. It is a form of secondary traumatic stress: you were not present for the original trauma, but repeated empathic engagement leaves you with symptoms similar to post-traumatic stress disorder (intrusive thoughts, hypervigilance, avoidance). Vicarious trauma is a related but distinct concept. It describes a cumulative shift in your worldview and identity, often after prolonged exposure to stories of human cruelty, systemic injustice, or loss. A child protective services worker may begin to perceive all parents as potential threats, or a refugee resettlement specialist may lose trust in institutions. Vicarious trauma changes how you see the world, not just how you feel at the end of a workday.
Why the Distinction Matters
The three conditions demand different responses. Burnout responds to organizational fixes: caseload caps, administrative support, flexible scheduling, and transparent promotion pathways. Compassion fatigue responds to clinical supervision, trauma-informed peer groups, and structured debriefing after difficult cases. Vicarious trauma may require individual therapy, a temporary leave, or a transition to a role with less direct trauma exposure. Many social workers experience all three simultaneously, which is why generic self-care advice (bubble baths, yoga, time off) rarely addresses the root causes. Effective prevention and intervention start with accurate assessment and a tailored strategy that matches the source of distress. Students entering the field can get a preview of these pressures through msw clinical year burnout patterns documented during supervised practice.
Burnout Vs. Compassion Fatigue Vs. Vicarious Trauma
Social workers frequently hear these three terms used interchangeably, but they describe distinct experiences with different causes, different recovery paths, and different implications for your career. Knowing which one you are dealing with is the first step toward addressing it effectively.
Burnout: A Workplace Problem
Burnout originates in the structure of the job itself. Excessive caseloads, inadequate resources, poor management, and a chronic mismatch between what you are asked to do and what you are equipped to do all drive burnout. That structural origin matters because it points directly to the solution: change the conditions. Research across mental health professions suggests burnout affects anywhere from 21% to 61% of practitioners, with rates among psychiatrists reaching as high as 78% and roughly half of behavioral health providers reporting burnout as of 2022.1 The primary workforce consequences are turnover and reduced capacity, which is why burnout registers as a top concern for employers in a way the other two conditions typically do not. With genuine workload reduction or a role change, burnout can resolve.
Compassion Fatigue: The Cost of Caring
Compassion fatigue develops through sustained empathic engagement with people in pain. It is less about how the organization is structured and more about the emotional labor of sitting with suffering day after day. Studies suggest that up to 70% of social workers experience compassion fatigue at some point in their careers, a figure consistent with broader estimates for helping professionals across the spectrum.1 The effects show up as reduced empathy and declining care quality, which hurt clients before they hurt the organization's numbers. Recovery is possible with deliberate self-care and peer support, but it rarely resolves on rest alone the way burnout can.2
Vicarious Trauma: A Shift in How You See the World
Vicarious trauma is the most persistent of the three. It results from repeated exposure to clients' traumatic material, and it does not simply lift when you take a vacation or switch roles.3 Research indicates that somewhere around 27% of helping professionals show symptoms consistent with post-traumatic stress, and career exposure estimates for vicarious trauma or compassion fatigue combined range from 40% to 85%.1 The damage is cognitive and existential: your worldview shifts, your judgment about safety and trust erodes, and clinical decision-making can suffer. Clinical practitioners in mental health settings carry higher risk than non-clinical leaders. Effective intervention requires trauma-informed supervision, not just stress management.
Why the Distinction Matters in Practice
Misidentifying the condition leads to the wrong remedy. A social worker who is vicariously traumatized will not recover by taking a week off. An organization that responds to systemic burnout by offering yoga classes is solving the wrong problem. Each condition calls for a targeted response, and understanding which one is driving your distress shapes everything from the support you seek to the conversations you have with supervisors.
How Common Is Burnout Across Social Work Fields?
Burnout is not distributed evenly across social work. Some specialties report crisis-level exhaustion, while others show more moderate strain. Nationwide, an estimated 62% of social workers have faced burnout in the past year, and rates of high emotional exhaustion exceed 70%.1 These averages, however, mask stark contrasts: child welfare and mental health settings consistently post the most alarming numbers.
The uneven landscape of burnout
Survey data from multiple studies paints a fragmented picture. Among all social workers, roughly 20% meet full burnout criteria, including depersonalization and reduced personal accomplishment.1 Yet in specific frontline roles, emotional exhaustion often surpasses 75%. The disconnect reveals that burnout is less about the profession and more about the conditions under which care is delivered.
Child welfare: the highest risk
Child welfare social workers face the most hazardous conditions of any subfield. Up to 75% of child protection social workers report high emotional exhaustion, and social workers serving disabled children reach 79%.1 Turnover rates in child welfare hover near 40% annually, and adoption workers average 55 cases, far beyond manageable thresholds.2 Mandatory investigation timelines, exposure to trauma, and moral distress from systemic constraints compound the pressure, driving experienced workers out of direct practice.
Healthcare and school settings under strain
Healthcare social workers face a different set of stressors: relentless discharge planning, ethical dilemmas, and the aftershocks of the pandemic. Burnout prevalence among health care staff overall declined from 49% in 2020 to 35% in 2023, but intent to leave remains high at nearly 29%.3 Meanwhile, among therapists including clinical social workers, 61% report emotional fatigue and 77% report mental fatigue.4 School social workers grapple with ballooning student mental health caseloads and severe underfunding, conditions tied to emotional fatigue even where specialty-specific data is sparse.
A workforce in retreat
Data from New Brunswick underscores the systemic nature of the crisis. Annual exits from practice doubled from about 5-6% before 2019 to roughly 10% after, and the share of social workers in frontline roles slipped from 73% to 67%.5 Many who leave eventually return, but the pattern suggests a cycle: burnout forces temporary withdrawal, thinning frontline ranks and adding pressure on those who remain.
Telehealth's double edge
The shift to remote services brought partial relief. Commute stress dropped, yet boundaries between work and home eroded. Many clinicians now report screen fatigue and a deeper sense of isolation, countering early hopes that online counseling and telehealth social work would ease emotional load. Without adequate organizational support, telehealth's net effect on burnout appears neutral at best, and in some settings it has accelerated feelings of disconnection.
Related Articles
Questions to Ask Yourself
Key Causes: Caseloads, Compensation, and Organizational Culture
Public child welfare agencies recommend caseloads of 15 to 20 families per worker, while private hospital systems typically cap clinical social work assignments at 12 to 18 active cases. In reality, frontline child welfare workers in many jurisdictions routinely carry 30 to 40 open cases, and hospital discharge planners manage panels that exceed 25 patients at peak census. That gap between recommended and actual workload is the single most consistent predictor of burnout across social work specialties.
Caseload Volume and Staffing Ratios
Unmanageable caseloads stem from chronic under-staffing, driven by budget constraints rather than evidence-based workforce planning. When a child welfare agency operates at 70 percent of authorized strength, remaining workers absorb the deficit. New hires inherit full caseloads within weeks, before they have mastered intake protocols or risk-assessment tools. High-volume environments leave no margin for unexpected crises, so workers skip lunch, work evenings, and defer documentation, which compounds stress and increases the likelihood of errors. The 2024 DataNB workforce study documented that frontline social work positions in New Brunswick declined from 73 percent to 67 percent of the registered workforce between 2010 and 2023, while exits from practice doubled from 5 to 6 percent before 2019 to roughly 10 percent after 2019.1 That attrition-driven staffing shortfall perpetuates a cycle in which remaining workers burn out faster, exit sooner, and leave even larger caseloads behind.
Compensation Relative to Emotional and Regulatory Demands
Nationwide, child, family, and school social workers earn a median annual wage of $58,570, with the middle 50 percent earning between $47,480 and $74,060. Healthcare social workers fare slightly better, with a median of $68,090 and a range from $55,360 to $83,410. While these figures exceed national median household income, they pale when weighed against the emotional intensity, regulatory liability, and advanced-degree requirements of the work. A hospital oncology social worker managing end-of-life care conferences, insurance denials, and family conflict earns less than many corporate human-resources generalists with bachelor's degrees. In high-cost urban markets, starting salaries in public child welfare often fall below the threshold needed to service graduate-school debt and afford rent, prompting early-career exits to adjacent fields such as program coordination or employee assistance, where work-life balance and pay improve.
Organizational Culture and Administrative Burden
Beyond caseload and pay, organizational culture is the third pillar of burnout risk. Inadequate clinical supervision, punitive management styles, and excessive documentation requirements erode worker morale and autonomy. Multiple time-use studies show that direct-service social workers spend 50 percent or more of their time on documentation, data entry, and compliance reporting, leaving less than half for face-to-face client contact, safety planning, or therapeutic intervention. When supervision focuses on audit compliance rather than reflective practice, workers lose the professional support needed to process vicarious trauma and refine clinical judgment. Agencies that treat workers as interchangeable case processors rather than autonomous professionals see higher turnover, lower job satisfaction, and elevated rates of sick leave. Workplace violence in social work compounds these pressures, adding a layer of physical and psychological risk that further strains retention. The "do more with less" ethos pervades public social services, where budget cuts are absorbed through attrition, hiring freezes, and workload redistribution rather than service reductions. That structural imbalance translates directly into individual burnout.
Social Worker Salary by Specialty: How Compensation Fuels Burnout
Compensation gaps across social work specialties help explain why burnout hits some fields harder than others. Child, family, and school social workers make up the largest segment of the profession yet earn the lowest median pay, a mismatch that compounds the emotional toll of high-caseload frontline work.

Warning Signs and Validated Assessment Tools
Twenty-two items across three subscales make the Maslach Burnout Inventory the most widely researched burnout measure in human services1, yet many social workers have never taken a validated assessment. Recognizing warning signs early and using evidence-based tools can mean the difference between course-correcting and leaving the profession entirely.
Symptoms Checklist: The Three Maslach Dimensions
Burnout presents differently across individuals, but validated research organizes symptoms into three core dimensions2:
- Emotional exhaustion: Chronic fatigue that sleep does not resolve, persistent insomnia, frequent illness or weakened immunity, feeling drained before the workday begins, and difficulty recovering energy during weekends or vacations.
- Depersonalization: Growing cynicism toward clients or the profession, emotional detachment during sessions, referring to clients by case numbers rather than names, and dark humor that crosses into contempt or callousness.
- Reduced personal accomplishment: Persistent feelings of ineffectiveness despite effort, questioning whether you chose the right career, inability to recall recent successes, and a sense that your work no longer matters.
If you notice symptoms across two or more dimensions lasting several weeks, a formal assessment offers clarity.
Three Validated Instruments Worth Knowing
Social workers have access to several validated tools, each with different costs, structures, and focal points:
- Maslach Burnout Inventory, Human Services Survey (MBI-HSS): Contains 22 items rated on a seven-point frequency scale (0 to 6).1 It measures emotional exhaustion, depersonalization, and personal accomplishment. The fourth edition removed fixed cutoff scores, encouraging users to interpret results relative to normative samples.3 Mind Garden, Inc. publishes the MBI, and licensing costs range from approximately $0.39 to $2.75 per administration depending on volume and format.4
- Professional Quality of Life Scale (ProQOL): A 30-item measure using a five-point Likert scale, assessing compassion satisfaction, burnout, and secondary traumatic stress.3 The ProQOL project makes this tool free for most uses, and it includes published cutoff thresholds for interpreting scores. Social workers can download it directly from the ProQOL website without licensing fees.
- Copenhagen Burnout Inventory (CBI): Developed by Kristensen and colleagues, this 19-item scale converts five-point responses to a 0 to 100 score across three subscales: personal burnout, work-related burnout, and client-related burnout.3 Thresholds are straightforward: 0 to 49 indicates low burnout, 50 to 74 moderate, 75 to 99 high, and 100 severe. The CBI is free for non-commercial use, making it accessible for agency-wide screening.
Practical Guidance: Administration, Frequency, and Interpretation
Most burnout instruments can be self-administered, though supervisors may incorporate them into scheduled check-ins for consistency. For individual practitioners, quarterly self-assessment provides a reliable baseline without assessment fatigue. Agencies conducting workforce wellness initiatives often administer tools annually or semi-annually.
When interpreting scores, the CBI offers the clearest thresholds: moderate scores (50 to 74) warrant attention to workload and self-care practices, while high scores (75 and above) signal the need for immediate intervention, whether through reduced caseloads, clinical supervision, or mental health resources for workers. The ProQOL similarly provides score ranges in its manual, helping users identify whether burnout or secondary traumatic stress is the primary concern.
Because the MBI no longer publishes fixed cutoffs, users compare their scores to normative data provided by Mind Garden.3 This approach offers nuance but requires more interpretive skill.
Choosing the Right Tool for Your Context
Budget often determines which instrument fits. If cost is a barrier, the ProQOL or CBI provides rigorous assessment at no charge. Agencies with research or accreditation requirements may prefer the MBI for its extensive validation history. For practitioners wanting to distinguish burnout from secondary traumatic stress or compassion fatigue, the ProQOL's three-subscale structure offers the most diagnostic clarity.
Regardless of which tool you select, the goal remains the same: quantify what you are experiencing so you can act on it. Scores are not verdicts but starting points for conversation, supervision, and strategic change.
Between 2010 and 2024, annual exits from social work practice in New Brunswick doubled from 5 to 6 percent before 2019 to roughly 10 percent afterward, while the share of workers in frontline roles fell from 73 to 67 percent. The data confirm that burnout is not simply pushing people out of the profession entirely but driving a mass retreat from direct practice into less demanding roles.
Evidence-Based Coping Strategies by Career Stage
Burnout prevention requires tailored interventions that match developmental readiness: the boundary-setting habits that protect an MSW intern differ from the structural advocacy that sustains a clinical supervisor. What works at one career stage may feel inaccessible or insufficient at another, so effective coping strategies are best organized by professional maturity.
MSW Students and Interns: Build Protective Habits Early
The field placement is your laboratory for boundary-setting, and missteps here seed burnout patterns that can persist for years. Establish clear working hours even when your supervisor models overwork, and communicate those limits explicitly during placement orientation. Peer debriefing groups (structured weekly check-ins with cohort members) provide a safe space to process difficult cases and normalize the emotional labor of learning. Reflective journaling, particularly after encounters that leave you depleted or activated, helps you track patterns before they calcify into chronic exhaustion. MSW field placement tips can reinforce many of these habits before you ever step into an agency. University of New Brunswick's "Wellbeing for Care Providers" course, developed by Dr. Leslie Jeffrey and Dr. Lisa Best, offers a replicable model: digital detox exercises and mindful walks are low-cost, evidence-informed practices that MSW programs can integrate into field seminar curricula.1 Students who adopt these habits during training report stronger retention and lower emotional exhaustion scores three years into practice.
Early-Career Practitioners: Systematize Self-Monitoring and Recovery
Your first post-degree role will test every boundary you set in school. Within your first 90 days, establish a relationship with an external clinical supervisor if your employer does not provide one; administrative supervision alone will not protect you from compassion fatigue. Use the Professional Quality of Life Scale (ProQOL) quarterly to track compassion satisfaction, burnout, and secondary trauma scores. Self-monitoring is most effective when it is scheduled and structured, not reactive. Create a "transition ritual" between work and home: a 10-minute walk, a change of clothes, or a deliberate closing of your case notes signals to your nervous system that the workday has ended. Mindfulness-based stress reduction (MBSR) has randomized controlled trial evidence for reducing emotional exhaustion in human service workers, and eight-week programs are now widely available online and in person.
Supervisors and Leaders: Model the Culture You Advocate For
If you hold supervisory responsibility, your burnout prevention work is structural. Model boundary-setting by leaving on time, taking your full lunch break, and explicitly naming when you decline after-hours requests. Advocate loudly for caseload limits in team meetings and budget discussions; your frontline staff cannot do this without career risk. Offer reflective supervision, not just administrative oversight: dedicate time in every session to emotional processing and meaning-making, not only case progress and documentation. Supervisors who normalize vulnerability and self-care create teams with measurably higher retention rates.
A Critical Caveat
These strategies buy time while systemic issues are addressed. Individual coping is necessary but insufficient. No amount of mindful walking will offset a 40-case load, poverty wages, or a director who punishes boundary-setting. Use these tools to sustain yourself, and channel the clarity they provide into collective advocacy for organizational change.
Organizational and Policy-Level Solutions That Actually Work
The conversation around social worker burnout has shifted decisively from individual coping to systemic accountability, with agencies, unions, and academic programs now treating workforce sustainability as an organizational design problem rather than a personal failing. The evidence backs this up: interventions that restructure workloads, supervision, and institutional culture produce measurable reductions in emotional exhaustion, and the effects are durable.
What the Research Shows About Organizational Interventions
A systematic review and meta-analysis of organizational workplace interventions in healthcare and helping professions found that, taken together, these strategies produced a modest but statistically significant reduction in emotional exhaustion (Cohen's d = -0.25, 95% CI: -0.37 to -0.13).1 Workload-specific interventions, such as caseload redistribution and scheduling reforms, showed a stronger effect on exhaustion (d = -0.44) than the average organizational approach.1 Most notably, combined interventions that paired workload changes with additional supports like peer consultation or process redesign yielded the largest effect (d = -0.54), and the benefits persisted for at least 12 months.1 Across 13 controlled studies of organizational interventions, 11 achieved significant burnout reductions.2 The takeaway is clear: agencies that invest in structural change rather than handing staff a self-care checklist get better results.
Caseload Caps and Collective Bargaining
Legislative and contractual caseload limits remain one of the most direct levers for reducing burnout. Several U.S. states have introduced or proposed caseload cap legislation for child welfare workers, and unionized social workers have used collective bargaining to negotiate enforceable limits alongside pay increases and safer working conditions. When caseloads are predictable and manageable, emotional exhaustion drops, turnover slows, and clients receive more consistent service. Unionization also provides a formal channel for frontline workers to advocate for policy changes, transforming individual frustration into collective structural pressure.
Reflective Supervision vs. Administrative-Only Models
Supervision quality matters as much as supervision frequency. Administrative-only supervision, focused on compliance, case documentation, and deadlines, does little to address the emotional toll of direct practice. Reflective supervision models, by contrast, create structured space for workers to process difficult cases, examine their emotional responses, and develop professional resilience. Evidence consistently links reflective supervision to lower emotional exhaustion scores and improved staff retention, particularly in child welfare and mental health settings. Agencies looking to curb burnout should ensure supervisors are trained in reflective practice rather than defaulting to a checklist-driven oversight model.
Pipeline-Level Prevention: Building Resilience Before Workers Enter the Field
One of the more forward-thinking approaches comes from the University of New Brunswick, which launched a BSW program on its Saint John campus in 2024. The first cohort graduated in spring 2026. A standout feature of the curriculum is a course called "Wellbeing for Care Providers," developed by faculty from history, politics, and psychology. It draws on neuroscience, contemplative studies, and practical techniques including digital detox exercises and mindful walks.3 The premise is simple: if social work programs equip students with evidence-based self-care habits before they encounter the pressures of frontline practice, those workers enter the field with a stronger foundation. DataNB workforce data from New Brunswick underscores the urgency: annual exits from social work practice in the province nearly doubled after 2019, rising from roughly 5 to 6 percent to about 10 percent.3 Integrating wellbeing training at the educational pipeline level is one replicable strategy for slowing that trend.
Participatory Approaches Deserve Attention
Another category worth highlighting is participatory interventions, where frontline staff help design the changes being implemented. These approaches produced meaningful reductions in exhaustion (d = -0.34, 95% CI: -0.47 to -0.20) across multiple studies,1 reinforcing what social workers already know from practice: people are more likely to engage with solutions they helped create. Agencies that invite staff input on workflow redesign, scheduling, and supervision formats build buy-in while generating solutions grounded in day-to-day reality.
For social workers evaluating potential employers or considering leadership roles, these data points offer a practical rubric. Agencies that combine workload reform, reflective supervision, and participatory decision-making are not just more humane workplaces. They are statistically more likely to retain their staff, protect service quality, and sustain the workforce that communities depend on. Social work research and practice offers additional frameworks for evaluating which organizational models have the strongest evidence base.
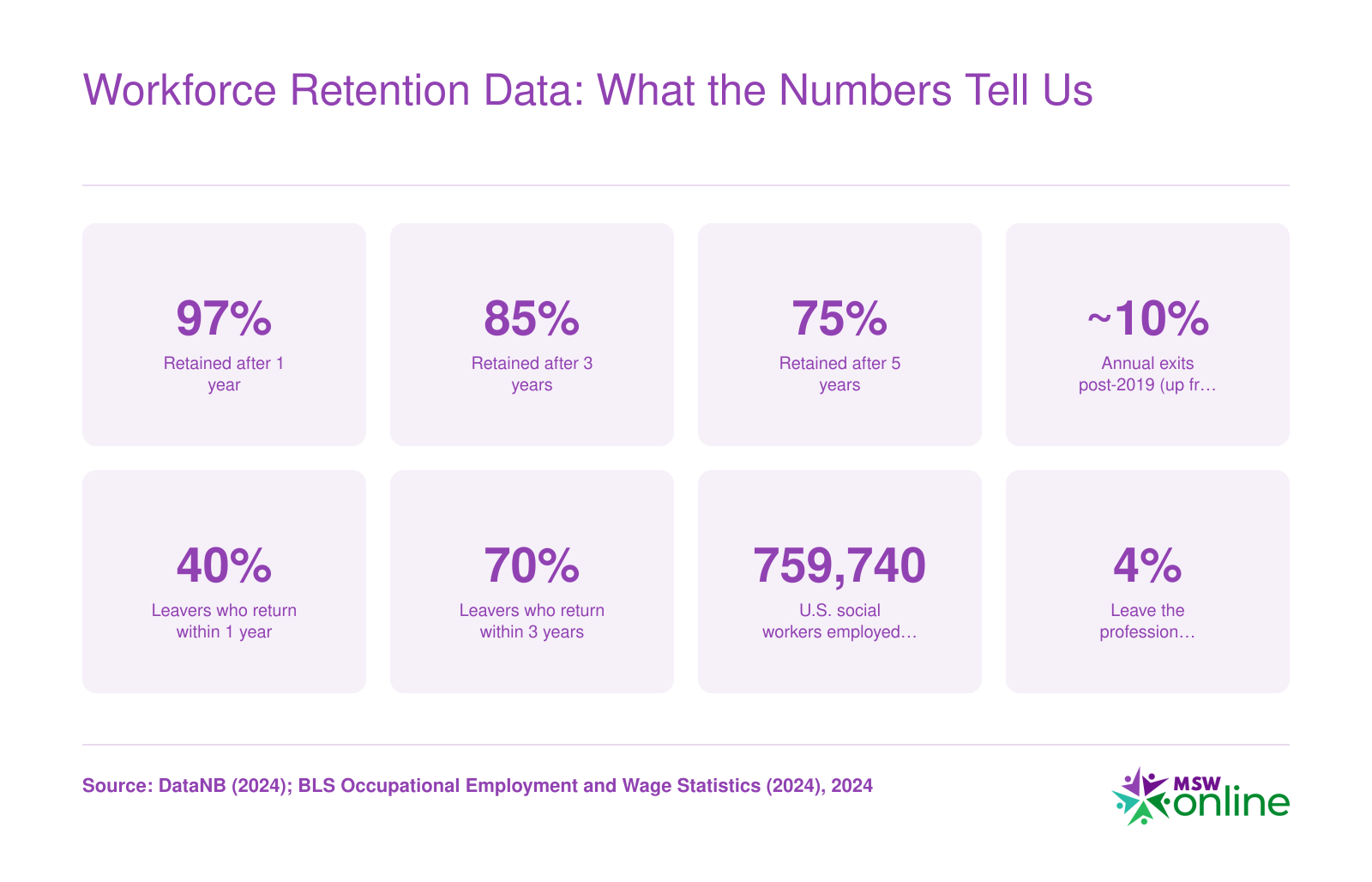
Workforce Retention Data: What the Numbers Tell Us
A 2024 DataNB study tracking New Brunswick social workers from 2010 to 2024 reveals that burnout-driven exits are accelerating, but many who leave eventually return. Nationally, the U.S. Bureau of Labor Statistics counts roughly 759,740 social workers employed across the country. When exit rates double, even temporarily, the ripple effects reach hundreds of thousands of practitioners and the communities they serve. The takeaway: departures are costly but often reversible when workplace conditions improve.
Building a Personal Burnout Prevention Plan
A mental checklist versus a written, structured plan: the difference between these two approaches often determines whether self-care stays aspirational or becomes routine. Social workers who commit their burnout prevention strategies to paper, revisit them monthly, and share them with a supervisor or accountability partner are far more likely to follow through than those who rely on good intentions alone.
Four Domains of a Written Prevention Plan
Organize your plan across four interconnected areas so that no single dimension of wellbeing is neglected.
- Physical: Set specific targets for sleep hygiene (consistent bedtime, no screens 30 minutes before sleep), weekly exercise frequency, and basic nutrition habits like meal prepping on weekends. Small, measurable commitments stick better than vague goals.
- Psychological: Schedule ongoing therapy or clinical consultation, even when you feel fine. Keep a reflective journal with brief end-of-day entries. Complete a Professional Quality of Life (ProQOL) self-assessment at least once per quarter to track changes over time before they escalate.
- Social: Identify a peer support group or regular check-in partner outside your immediate team. Protect your supervisory relationship as a clinical resource, not just an administrative requirement. Maintain friendships and community ties that have nothing to do with social work.
- Spiritual and meaning-making: Reconnect with the reasons you entered the profession. Consider volunteering in a capacity unrelated to your paid role to restore a sense of agency. Incorporate contemplative practices, whether meditation, prayer, or quiet reflection, into your weekly routine.
Micro-Practices Worth Borrowing
The University of New Brunswick's "Wellbeing for Care Providers" course, developed by faculty in psychology and history/politics, offers two daily practices that any social worker can adopt immediately: scheduled digital detox periods (even 20 minutes with your phone in another room) and mindful walks between appointments or during lunch.1 These are not luxuries. They are evidence-informed resets rooted in neuroscience and contemplative studies, and they require no budget or organizational approval.
Revisit, Share, and Advocate
Treat your plan like a living document. Block 30 minutes on the first of each month to review what is working and where you have slipped. Share relevant sections with your supervisor or an accountability partner so someone else can flag warning signs you might miss.
One final, essential point: a personal prevention plan is a complement to organizational advocacy, never a replacement for it. Individual resilience cannot compensate for unsustainable caseloads, inadequate pay, or toxic workplace culture. While you protect your own wellbeing, continue pushing for systemic changes, such as better staffing ratios, livable compensation, and strengths-based assessment tools that support sustainable supervision models, to reduce the conditions producing burnout in the first place. Both efforts are necessary, and neither is sufficient on its own.
Frequently Asked Questions About Social Worker Burnout
These answers address the most common questions about social worker burnout, from prevalence data to prevention strategies. Each response draws on research and workforce data discussed throughout this guide. For a deeper look at any topic, follow the references to the relevant sections above.