Points of interest…
- Nearly 70 percent of all mental health professional shortage areas are located in rural communities across the United States.
- The NHSC Loan Repayment Program offers up to $50,000 for licensed clinical social workers serving in eligible rural sites.
- Online MSW programs let rural residents complete field placements locally, training in the communities where demand is greatest.
- By 2021, 55 percent of rural residents had used telehealth for a mental health visit, reshaping service delivery nationwide.
Nearly 60 million Americans live in rural areas, yet these communities face a social worker-to-population ratio dramatically lower than their urban counterparts. More than two-thirds of designated mental health professional shortage areas are rural, and only about one quarter of behavioral health workforce needs are being met in those regions. The gap is both a hiring crisis and a pipeline problem: most MSW programs concentrate their students and field sites in urban centers, even as demand for rural clinicians climbs.
The staffing imbalance shapes every aspect of rural practice. A social worker in a rural county routinely juggles child welfare and geriatric case management alongside mental health crisis response, often as the only licensed clinician within a 60-mile radius. Salary data, loan forgiveness mechanisms, telehealth policy, and MSW curriculum design all influence whether new graduates will serve in these high-need areas. Federal loan repayment programs now cover up to $75,000 for clinicians who commit to underserved sites, and online MSW tracks have made it possible to earn a degree without relocating to a university town.
What Is Rural Social Work?
Urban social workers typically specialize in one population or service area; rural social workers do the opposite, often serving as the only licensed clinician within a 60-mile radius and handling everything from child protection intakes to elder care coordination in a single workday. That breadth defines the field.
How "Rural" Is Defined
The U.S. Census Bureau classifies any area outside an urbanized cluster of 50,000 or more as rural, while the USDA Rural-Urban Continuum Codes break this down further into nine tiers ranging from metro-adjacent counties to completely isolated frontier areas. In practice, rural social work spans three distinct settings:
- Small towns and farming communities: Populations under 25,000, often county seats serving surrounding agricultural land.
- Frontier areas: Fewer than six people per square mile, common across the Mountain West and Alaska.
- Tribal communities: Reservations and Native villages with sovereign governance, unique federal service structures, and distinct cultural protocols.
Generalist Practice, Not Specialist
Rural practitioners are generalists by necessity. One worker may carry a caseload that includes a teenager in substance abuse social work, an aging farmer refusing in-home care, a veteran navigating PTSD, and a family applying for SNAP, all in the same week. Referrals to specialists are limited, so rural social workers rely on informal community networks: pastors, school nurses, county extension agents, and neighbors. Client relationships tend to run deeper and longer than in urban caseloads, partly because anonymity is impossible and partly because continuity is the only viable model.
Who Rural Social Workers Serve
Core populations include agricultural and migrant workers, Native and Indigenous communities, elderly residents aging in place, returning veterans, and families living below the poverty line. These groups face documented mental health disparities: rural suicide rates run roughly 25 percent higher than urban rates per CDC data, and behavioral health access lags sharply behind metro areas. VA social work careers offer one avenue for reaching veterans in these underserved communities. Demand is highest precisely where the workforce is thinnest, the workforce gap this guide examines next.
Rural Social Work Shortage: How Severe Is the Problem?
The rural social work shortage has reached crisis proportions, with nearly 70 percent of all mental health professional shortage areas located in rural communities and only about one quarter of the nation's mental health workforce needs being met in those areas.
Mental Health Professional Shortage Areas in Rural America
As of April 2026, the Health Resources and Services Administration designated 6,959 mental health Health Professional Shortage Areas across the United States.1 Of those, 4,759 are rural designations, meaning that nearly 68 percent of all mental health HPSAs serve rural populations.1 These designations are not merely administrative labels. They signal that communities lack sufficient licensed providers to meet basic mental health service demand. Nationwide, more than 137 million people live in designated mental health HPSAs, and current providers meet only 27 percent of the calculated need.2 HRSA estimates that an additional 6,800 mental health practitioners would be required to eliminate the shortage, and a disproportionate share of that gap sits in rural counties.2
Vacancy Rates and Time to Fill Rural Positions
Rural social service agencies report persistently higher vacancy rates and longer recruitment timelines than their urban counterparts. Workforce studies conducted by the National Association of Social Workers have documented that rural positions often remain open for months, forcing remaining staff to carry unsustainable caseloads. Agencies in micropolitan and noncore counties struggle to attract early-career professionals, who often gravitate toward metropolitan markets with higher salaries, professional development resources, and peer networks.
Demand Drivers Compounding the Shortage
Several converging trends are intensifying rural demand for social workers. The Bureau of Labor Statistics projects steady growth in social work employment through the end of the decade, driven in part by an aging population that requires elder care coordination and chronic disease management. Rural America skews older, with median ages in many counties exceeding the national average by five to ten years. At the same time, the opioid crisis continues to extract a toll on rural families, generating sustained need for substance abuse social workers and child welfare professionals. Agricultural communities face a parallel mental health emergency, with farm stress and suicide rates elevated by volatile commodity prices, climate variability, and intergenerational land transfer pressures.
The Retirement Cliff
Adding urgency to these demand drivers is the looming retirement cliff. A significant portion of the rural social work workforce is age 55 or older, and many practitioners plan to retire within the next five years. Without a robust pipeline of new graduates willing to practice in rural settings, agencies will struggle to maintain even current service levels, let alone expand to meet growing need.
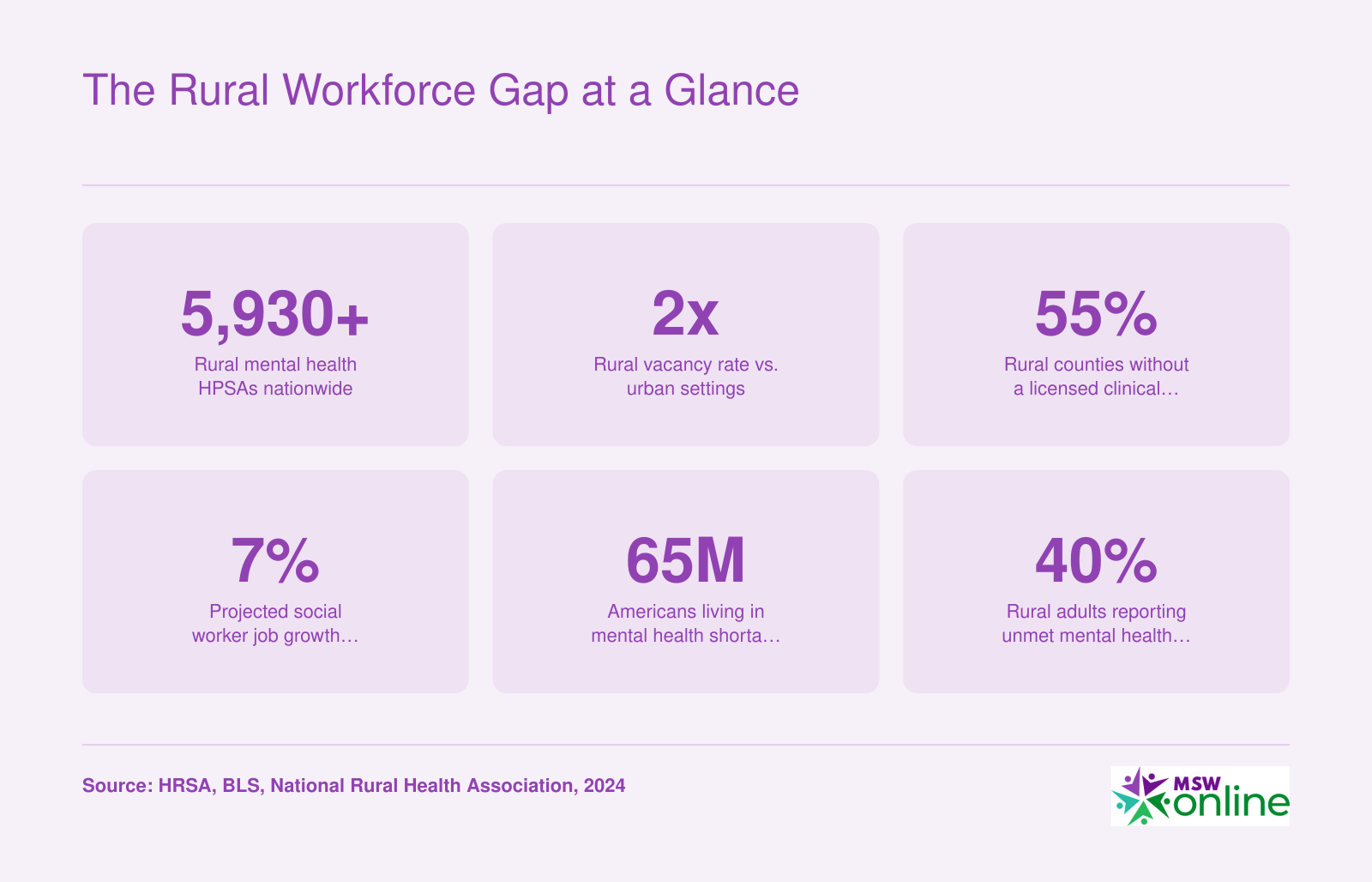
The Rural Workforce Gap at a Glance
Rural communities face persistent shortages of behavioral health professionals, and the gap continues to widen. These figures illustrate the scale of the crisis and why targeted workforce strategies are urgently needed.
Key Challenges of Rural Social Work Practice
A systematic review of 28 studies on rural social work found that approximately 13 percent of rural social workers report high risk for compassion fatigue and burnout, highlighting the unique stressors of practicing in sparsely populated communities.1 While rural social work offers deep community ties and meaningful relationships, it also presents operational and ethical challenges rarely encountered in urban settings.
Dual Relationships and Boundary Management
In a town of 2,000 people, your client may also be your neighbor, your child's teacher, or the person ringing up your groceries at the local market. These dual relationships are not occasional accidents but the structural reality of rural practice. The code of ethics social work discourages dual relationships when they risk harm or exploitation, yet avoiding them entirely in small communities is often impossible. Social workers must navigate confidentiality when running into clients at church, school events, or the only restaurant in town. This ethical complexity requires constant vigilance, clear boundaries, and transparency with clients about the realities of small-town life. Unlike urban practitioners who can maintain anonymity outside the office, rural social workers live and work in overlapping social circles, making every public interaction a potential professional concern.
Professional Isolation and Limited Supervision
Rural social workers often practice alone or in very small teams, with limited access to specialized consultation or peer supervision. Research shows that supervisory support is a key protective factor for retention in rural settings,2 yet many practitioners work in agencies with no on-site MSW supervisor or in solo private practices with no colleagues nearby. This isolation extends to continuing education: traveling three or four hours to attend a training on trauma-informed care or substance use disorders is common. Without regular peer support, the risk of burnout increases. Studies examining age and burnout in rural child welfare workers found coefficients ranging from negative 0.39 to negative 0.40, indicating that younger workers face higher burnout risk, possibly because they lack the professional networks and coping strategies that come with experience.3
Resource Scarcity and Creative Problem-Solving
Rural social workers frequently operate in environments where the nearest psychiatric hospital is 100 miles away, affordable housing for clients in crisis does not exist, and referral networks are thin or nonexistent. There may be no psychiatrist in the county, no domestic violence shelter, and no public transportation. This scarcity demands creativity: a social worker might collaborate with a pediatrician to manage a child's anxiety because no child therapist is available, or help a client access remote resources for mental health workers because in-person specialists are out of reach. Poor job satisfaction, linked to inadequate resources and high caseloads, is a strong predictor of turnover in rural settings.2
Travel Burden and Geography
Large service areas mean rural social workers routinely drive 50 to 100 miles between home visits. Weather conditions, unpaved roads, and seasonal hazards add unpredictability and risk. A winter storm can cancel a day's appointments or strand a worker miles from the office. Time spent driving is time not spent with clients, yet it is an unavoidable cost of serving dispersed populations.
Stigma and Cultural Barriers to Seeking Help
Rural cultural norms often emphasize self-reliance, privacy, and skepticism of outsiders, including mental health professionals. Clients may resist seeking help because they fear being recognized at the social services office or because asking for assistance contradicts deeply held values. Confidentiality becomes more fraught when everyone knows everyone, and word of a therapy appointment can travel quickly through informal networks. Social workers must work harder to build trust, normalize help-seeking, and respect the cultural contexts that shape client behavior.
Questions to Ask Yourself
Rewards and Benefits of Working in Rural Communities
Rural social work is experiencing a surge in interest among practitioners seeking deeper engagement and broader autonomy than urban bureaucracies typically allow. While much of the literature on rural practice emphasizes shortages and hardships, the day-to-day reality for many rural social workers includes professional freedoms, visible community impact, and quality-of-life factors that urban roles rarely match.
Autonomy and Professional Breadth
Rural social workers develop a wider skill set than their urban counterparts, often by necessity. In a county with one social worker covering child welfare social work, mental health, and aging services, you become a generalist by default. This breadth translates into greater decision-making authority: you are not one tier in a multi-layer agency hierarchy. You assess, plan, and execute interventions with minimal bureaucratic delay, and supervisors are more likely to trust your clinical judgment when you are the only licensed professional within 50 miles.
Visible Community Impact
In a community of 2,000, there is no anonymity in impact. You see the teenager you placed in foster care graduate high school. You run into the family you connected to housing assistance at the grocery store. This visibility cuts both ways, but many practitioners find it profoundly meaningful: your work is woven into the fabric of the community, not abstracted into case counts and quarterly metrics.
Deeper Client Relationships and Continuity of Care
Rural practice allows you to follow families over years, not episodes. You are not handing off a case file every six months when a client's insurance changes or they move across a district boundary. Continuity of care is the default, and many social workers report that these long-term relationships are the most rewarding aspect of rural work, offering insight into intergenerational patterns and the chance to witness real transformation over time.
Lower Cost of Living and Quality-of-Life Factors
Rural placements often come with lower housing costs, shorter commutes, and access to outdoor recreation that urban salaries cannot buy. A $52,000 salary in rural Montana or eastern Kentucky may afford a quality of life equivalent to $75,000 in Denver or Charlotte. Less time in traffic means more time with family or on trails, and many practitioners cite this balance as a primary reason they stay.
Financial Incentives
Loan forgiveness programs, signing bonuses, and housing stipends specifically target rural placements, and these incentives can narrow or eliminate the salary gap with urban roles. Social work grants for practitioners are another funding avenue worth exploring alongside these programs. We cover loan forgiveness in detail in the next section, but it is worth noting that the total compensation package in rural settings often exceeds the base salary alone.
Rural Vs. Urban Social Work Salaries
Salary comparisons between rural and urban settings are nuanced. The Bureau of Labor Statistics does not break out wages by rural versus urban designation directly, but state-level data offers useful context. States with large rural populations often report lower median wages than heavily urbanized states, though the gap is smaller than many candidates expect, especially after factoring in lower costs of living. The table below compares median annual wages across social work specialties in states that range from predominantly rural to predominantly urban, based on 2024 Occupational Employment and Wage Statistics from the U.S. Bureau of Labor Statistics.
| State | Setting Profile | Child, Family, and School Social Workers (Median) | Healthcare Social Workers (Median) | Social Workers, All Other (Median) |
|---|---|---|---|---|
| California | Highly urban | $69,250 | $92,970 | N/A |
| New York | Highly urban | $65,430 | N/A | N/A |
| Connecticut | Urban | $78,940 | $81,900 | N/A |
| New Jersey | Urban | $78,150 | $81,710 | N/A |
| District of Columbia | Urban | $78,920 | $92,600 | N/A |
| Maryland | Mixed | $70,840 | N/A | $77,900 |
| Washington | Mixed | $72,290 | $75,670 | $96,550 |
| Minnesota | Mixed | $65,010 | $72,330 | $79,220 |
| Colorado | Mixed | $63,560 | N/A | N/A |
| Virginia | Mixed | N/A | N/A | $86,690 |
| Indiana | More rural | N/A | N/A | $80,410 |
| Iowa | More rural | N/A | N/A | $88,000 |
| Vermont | Predominantly rural | $65,370 | $78,390 | N/A |
| New Hampshire | Predominantly rural | $64,630 | $78,000 | N/A |
| North Dakota | Predominantly rural | $66,900 | N/A | $77,380 |
| South Dakota | Predominantly rural | N/A | N/A | $89,320 |
| Mississippi | Predominantly rural | N/A | N/A | $89,860 |
| Alabama | Predominantly rural | N/A | N/A | $89,170 |
| Maine | Predominantly rural | N/A | $72,520 | N/A |
| Alaska | Predominantly rural | N/A | $77,990 | N/A |
Salary Snapshot: What Social Workers Earn Nationally
National wage data for social workers shows a broad earnings range depending on specialty, setting, and geography. Rural salaries tend to cluster closer to the 25th percentile, but lower housing costs, shorter commutes, and reduced everyday expenses in rural areas narrow the real purchasing-power gap significantly.

How MSW Programs Are Addressing Rural Workforce Shortages
Graduate social work education has historically concentrated students in urban areas, but a growing number of MSW programs now build rural practice into their curriculum, field placements, and recruitment strategies. These efforts aim to prepare students for the realities of rural service delivery while keeping them connected to the communities that need them most.
Programs With Dedicated Rural Concentrations
Several accredited MSW programs offer explicit rural tracks that go beyond electives to provide comprehensive preparation for practice in underserved areas:
- Stephen F. Austin State University (Texas): Offers an Advanced Generalist Practice in a Rural Context concentration through its online advanced standing track. The curriculum addresses the unique challenges of serving geographically dispersed populations in East Texas and similar regions.1
- Concord University (West Virginia): The online MSW features an Advanced Generalist Practice with Specialization in Rural Practice, designed for a state where nearly all counties qualify as rural or medically underserved.2
- Arkansas State University: Provides a Rural Based Clinical Social Work Practice with an Emphasis on Trauma-Informed Care concentration, acknowledging that rural communities often experience higher rates of trauma with fewer treatment resources.
- Cal Poly Humboldt (California): The Distributed Learning MSW emphasizes Working in Rural and Indigenous Communities, recognizing the overlap between geographic isolation and service gaps affecting tribal populations.
- Ohio University: Offers Clinical Social Work with an Emphasis on Service in Rural Environments, targeting Appalachian communities across southeastern Ohio.
- West Virginia University: The MSW concentration in Advanced Integrated Practice with Emphasis on Rural Service Delivery prepares students for multi-role positions common in small agencies.
Rural Field Placement Pipelines
These programs do not simply teach about rural practice; they partner with rural agencies to place students directly in underserved communities during practicum. The goal is straightforward: students who complete placements in rural settings are far more likely to accept jobs there after graduation. By building relationships with federally qualified health centers, community mental health agencies, school districts, and tribal organizations, programs create pipelines that convert interns into long-term hires.
Grow-Your-Own Recruitment Models
Some programs recruit students who already live in rural areas and train them to remain. This approach, sometimes called a grow-your-own model, recognizes that retention improves when practitioners have existing roots in a community. Stipend-supported cohorts, partnerships with community health worker programs, and targeted scholarships for rural residents all reduce the financial barriers that push students toward urban jobs after graduation.
Online Delivery as an Access Strategy
All six programs listed above offer fully online MSW programs or distributed learning options. This design is intentional: students can earn their MSW without relocating to a campus city, maintaining their connections to family, employment, and community. Online delivery removes one of the largest structural barriers to increasing the rural workforce, because students who never leave are more likely to practice where they already live.
If you are weighing which program fits your situation, choosing the right online MSW program involves comparing field placement logistics, rural concentration options, and financial support structures alongside the usual factors of cost and accreditation. Published outcome data on graduate retention in rural areas remains limited, but early indicators suggest that programs combining rural concentrations, local placements, and online delivery produce higher rates of graduates working in shortage areas compared to traditional campus-based programs without these features.
Online and hybrid MSW programs allow rural residents to earn a graduate degree without relocating to urban university centers. Field placements can often be completed at local agencies, hospitals, or community organizations, meaning students train in the very settings where they are most needed. This model creates a direct pipeline: students remain rooted in their communities and frequently stay after graduation, addressing workforce shortages from within.
Loan Forgiveness and Financial Incentives for Rural Social Workers
Federal and state loan repayment programs are reshaping where new social workers choose to practice, making rural service more financially viable than ever. For licensed clinical social workers, the National Health Service Corps (NHSC) Loan Repayment Program offers up to $80,000 for a two-year full-time commitment in a designated Health Professional Shortage Area (HPSA), with higher HPSA scores boosting selection priority.1 Part-time options and continuation awards further extend the benefit, creating a powerful recruitment tool for underserved communities.
NHSC Programs Tailored to Rural and High-Need Settings
The standard NHSC Loan Repayment Program requires 32 hours per week of direct patient care for two years, with the $80,000 award applied directly to qualifying educational loans.2 Social workers who serve half-time (16 to 31 hours weekly) can receive proportionally smaller awards. After the initial contract, continuation funding of $20,000 per year is available for those who extend their service, and a $5,000 Spanish language enhancement is added for providers serving patients in Spanish.3 For social workers focusing on substance use disorders, the NHSC Substance Use Disorder Workforce Loan Repayment Program provides up to $75,000 for three years, while the NHSC Rural Community Loan Repayment Program specifically targets rural opioid and SUD treatment with a $100,000 award over three years.4 All programs require U.S. citizenship or national status.3
Public Service Loan Forgiveness for Rural Practitioners
Many rural social workers are employed by qualifying nonprofits or government agencies, such as community health centers, school districts, or county mental health departments. These positions typically meet the employer requirement for Public Service Loan Forgiveness (PSLF), which discharges the remaining balance on federal Direct Loans after 120 qualifying monthly payments. Because PSLF is not capped and is tax-free, a social worker who consolidates loans early and stays in qualifying employment while making income-driven payments can see tens of thousands of dollars forgiven after 10 years. The key is to submit the Employment Certification Form annually to track progress.
State-Specific Incentives Deepen the Pool of Support
Many states operate their own loan repayment or incentive programs to address local shortages, often stacking with federal options. Colorado's Health Service Corps, for example, offers competitive awards for two-year commitments in underserved areas, with priority for rural sites. Minnesota's loan forgiveness program for mental health professionals includes designated rural regions and can provide substantial annual disbursements. Alaska's SHARP (Supporting Health Access in Rural Practices) program targets behavioral health clinicians with multiyear service agreements, and Montana's Rural Physician Incentive Program now extends to licensed clinical social workers, offering sizable payments toward student loans. Each program sets its own award caps, service obligations, and employer eligibility, so candidates should research options in their intended practice state.
Scholarships and Stipends That Reduce Upfront Debt
Beyond loan repayment, forward-looking financial aid can lighten the debt burden before it starts. The Council on Social Work Education (CSWE) administers minority fellowships for social work students committed to underserved populations, including rural areas. HRSA's behavioral health workforce education and training grants fund dozens of MSW programs that place students in rural internships and often include tuition support or living stipends. Individual universities also earmark MSW scholarships for students pledging to practice in rural settings post-graduation, and the Indian Health Service offers scholarship and loan repayment programs for providers serving American Indian and Alaska Native communities, many of which are rural.
Stacking Benefits for Maximum Relief
The combined power of these programs can be transformative. A social worker who secures an NHSC award, works in a PSLF-eligible setting, and supplements with a state repayment grant could eliminate well over $100,000 in student debt over a decade. For example, the $80,000 NHSC award alone covers much of a typical MSW graduate's federal loans, while PSLF handles the remainder after 10 years. When state programs add another $20,000 to $50,000, the total relief easily reaches six figures, making a rural career not only mission-driven but also financially sustainable. Careful planning with a tax advisor and annual recertifications are essential to maximize all available avenues.
Telehealth, Technology, and the Future of Rural Social Work
Telehealth in social work means delivering counseling, case management, crisis intervention, and clinical supervision through video, phone, or secure messaging platforms, connecting practitioners and clients who would otherwise be separated by geography, transportation barriers, or provider shortages.
How COVID Accelerated Adoption
Before 2020, behavioral health telehealth was the exception rather than the rule. In 2015, fewer than one in four mental health treatment facilities (22.2%) and roughly one in four substance use treatment facilities (25.7%) reported offering telemedicine services at all, according to data from the Substance Abuse and Mental Health Services Administration.1 The pandemic changed that trajectory almost overnight. Among rural Medicare beneficiaries, telehealth utilization reached 44 percent between March 2020 and February 2021, a figure that would have been unthinkable just five years earlier.2 Urban utilization ran somewhat higher at 55 percent over the same period, partly because urban residents have historically had more experience navigating digital health platforms.2 Regardless, the shift signaled that rural clients and providers could and would embrace remote care when in-person access collapsed.
Tele-Supervision: Closing the Mentorship Gap
One underappreciated benefit of telehealth technology is tele-supervision, which allows newly licensed or pre-licensed social workers in isolated communities to receive regular clinical oversight from experienced supervisors located anywhere in the country. Rural practitioners have historically struggled to accumulate the supervised hours required for licensure simply because qualified supervisors were not nearby. Remote supervision platforms are dismantling that barrier, reducing geographic isolation as a reason that early-career social workers leave rural positions.
Some MSW programs are beginning to embed this reality into their curricula. The University of North Carolina's School of Social Work, for example, has drawn attention for its commitment to rural health equity, and a growing number of online counseling and tele-social work programs now include coursework on digital ethics and remote engagement skills.
Barriers That Technology Cannot Yet Solve
Progress is real, but uneven. Approximately 28 percent of rural residents lacked reliable broadband access as recently as 2022, and the figure reaches 24 percent in tribal areas.2 Spotty connectivity makes video-based sessions unreliable or impossible for some of the clients who need services most. Beyond infrastructure, certain client populations, particularly older adults and those with limited digital literacy, may find video platforms alienating. Resources addressing how to combat social isolation in seniors can inform practitioners working with this demographic in low-connectivity settings. Regulatory complexity adds another layer: telehealth licensure rules vary by state, meaning a social worker in one state cannot always serve a client just across the border without navigating a different licensing authority.
What Comes Next
Looking ahead, the tools available to rural practitioners are expanding beyond video calls. AI-assisted screening tools are being piloted to help flag clients at elevated risk for depression, substance use, or housing instability before a crisis develops. Digital case management platforms can centralize client records, appointment scheduling, and service referrals in ways that reduce the administrative burden that often falls disproportionately on solo rural practitioners.
None of these technologies replace the trust built through in-person community presence, which remains a cornerstone of effective rural social work. The more realistic and sustainable vision is a hybrid model: technology handles routine check-ins, documentation, and distance supervision, while in-person visits are reserved for the situations where physical presence matters most. That balance, rather than a fully virtual future, is where the field is heading.
Before the pandemic, tele-mental health was rare in rural areas. By 2021, however, 55% of rural residents had used telehealth for a mental health visit, according to a Kaiser Family Foundation analysis. This rapid increase underscores how virtual care is helping to close the rural mental health gap.
Common Questions About Rural Social Work
Below are answers to the questions prospective rural social workers ask most often. Each response offers a concise overview; scroll to the corresponding section earlier in this guide for full details, statistics, and resource links.
Related Articles
Specialized urban practice versus generalist rural service: that is the fork in the road for many new MSWs. If you choose rural, you step into a field with historically high demand, expanding financial incentives, and technology tools that now make even remote communities accessible to clinical supervision and peer networks. The workforce gap remains a crisis, but it is also a career opportunity for social workers willing to invest in underserved areas where they will often be the only licensed professional within sixty miles.
Start by exploring MSW programs with rural tracks or field placements in frontier settings. Check NHSC Health Professional Shortage Area eligibility for your target county, and connect with your state's workforce board to learn about sign-on bonuses, loan repayment, and tax credits. For practitioners concerned about personal safety in isolated assignments, social worker safety tips offer practical guidance worth reviewing before your first rural placement. The infrastructure to support rural social workers exists today in a way it did not five years ago.