Points of interest…
- Roughly two in three adults experiencing homelessness meet criteria for at least one mental health disorder.
- Black Americans represent about 13% of the U.S. population but account for 37 to 40 percent of those experiencing homelessness.
- Housing First models consistently reduce chronic homelessness while improving psychiatric outcomes across multiple controlled studies.
- About 70% of uninsured homeless individuals eligible for Medicaid face enrollment barriers that block mental health access.
On a single night in January 2024, HUD counted more than 770,000 people experiencing homelessness in the United States, the highest figure since point-in-time tracking began. Roughly a third reported a serious mental illness or substance use disorder, and the causation runs both directions: untreated psychiatric conditions destabilize housing, and the trauma of living unsheltered worsens existing symptoms.
For social workers, that bidirectional loop shapes nearly every decision in the field, from intake triage to long-term case planning. The clinical picture, the intervention models (Housing First, ACT, critical time intervention), the credentialing path, and the wage spread across settings all sit inside that loop. Professionals considering specializations such as mental health and substance abuse social workers will find this population at the center of their caseloads.
Federal funding for permanent supportive housing has plateaued while shelter demand keeps climbing, reshaping where new positions open and what caseloads look like.
Understanding the Link Between Mental Health and Homelessness
How exactly do mental health conditions and homelessness feed into each other?
A Two-Way Street: Mental Health as Cause and Consequence
For many individuals, untreated mental illness precipitates the loss of employment, social support, and housing. Serious psychiatric symptoms can disrupt one's ability to maintain relationships, manage finances, or keep a steady job. Once homelessness sets in, the environment itself compounds the damage. Constant exposure to danger, sleep deprivation, extreme weather, and stigma creates chronic stress that accelerates psychiatric decline. A 2024 systematic review in JAMA Psychiatry pooled data from 85 studies and over 48,000 participants, finding that 67% of homeless individuals had a current mental health disorder.1 In North America, lifetime prevalence reached 77%.1 The U.S. Department of Housing and Urban Development's annual Point-in-Time count reports that 25% to 30% of sheltered homeless persons experience serious mental illness, and a similar proportion struggles with chronic substance use. This two-way dynamic means that addressing one side without the other is rarely effective.
Prevalence of Specific Diagnoses
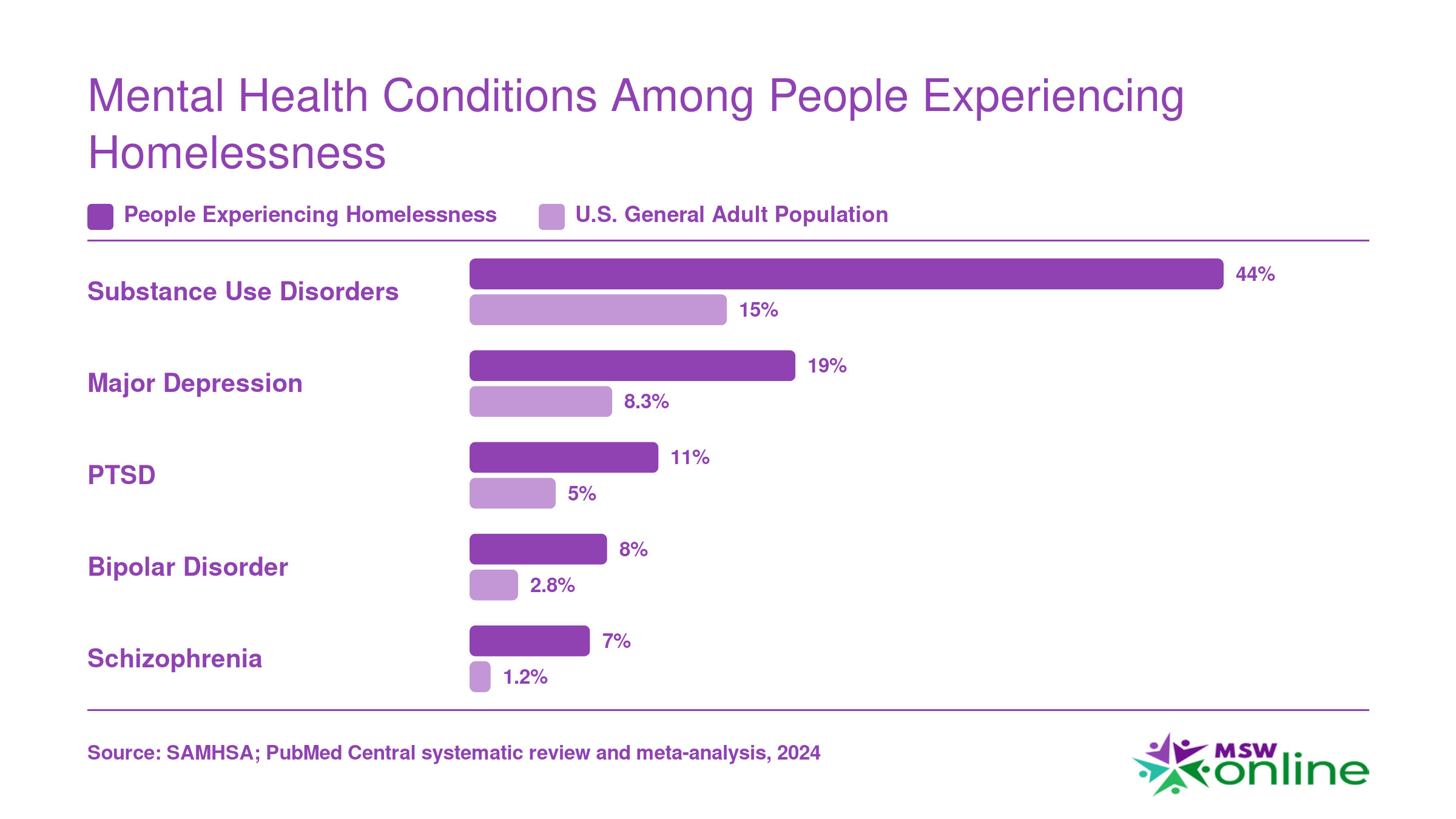
The same 2024 meta-analysis provides a detailed diagnostic breakdown. Among people experiencing homelessness:
- Major depressive disorder: 19% currently affected.1
- Any psychotic disorder: 14% (with schizophrenia specifically at 7%).1
- Bipolar disorder: 8% currently.1
- Post-traumatic stress disorder (PTSD): 11% currently.1
- Substance use disorder: 44% currently, with lifetime rates at 56%.1
These figures far exceed rates in the general population. For context, lifetime prevalence of schizophrenia in the general U.S. population is about 1%. The elevated 7% rate among homeless samples underscores the strong link between severe mental illness and housing instability. Traumatic brain injury, though less consistently measured, also appears disproportionately high and is associated with behaviors that raise homelessness risk, including impulsivity and aggression. The breadth of these conditions illustrates why effective interventions must be comprehensive, and why professionals pursuing careers in social work in mental health need training that spans multiple diagnoses.
Conditions That Precede Versus Follow Homelessness
Not all psychiatric disorders emerge from the same pathway. Schizophrenia and other psychotic disorders typically onset in late adolescence or early adulthood, before most individuals first experience homelessness. These disorders are a primary driver of initial housing loss due to their impact on functional capacity and social relationships. By contrast, PTSD and major depression frequently develop or worsen after entry into homelessness. The everyday trauma of living on the streets, including assault, theft, and constant vigilance, provides fertile ground for stress-related disorders. A person who was previously stable may develop depression or anxiety as a direct result of their circumstances. Bipolar disorder can both precede homelessness and be exacerbated by it; manic episodes may go untreated without access to care, leading to eviction, while the stress of homelessness may trigger new mood cycles. Recognizing this temporal difference matters because prevention and intervention strategies differ: early treatment for schizophrenia might forestall homelessness, whereas trauma-informed care and safe housing can mitigate PTSD.
Substance Use and Dual Diagnosis
Roughly half of homeless individuals who have a mental illness also have a co-occurring substance use disorder, a situation known as dual diagnosis. The 2024 JAMA study reported a current substance use disorder prevalence of 44%, and lifetime rates of 56%.1 Alcohol use disorder and drug use disorder often intertwine with mental illness in a self-medicating cycle: a person drinks or uses drugs to dull psychiatric pain, but substance use then deepens mood instability and impairs decision-making, making it harder to engage with treatment or keep appointments. Practitioners trained as substance abuse social workers play a critical role in breaking this cycle. Dual diagnosis is particularly challenging to manage in traditional shelter systems where mental health and addiction services are siloed. Integrated treatment models that address both conditions simultaneously are considered best practice, though they remain scarce in many communities.2 Without coordinated care that treats the whole person, individuals often cycle repeatedly between shelters, hospitals, and the streets.
Mental Health Conditions Among People Experiencing Homelessness
Roughly two in three adults experiencing homelessness meet criteria for at least one mental health disorder, nearly triple the rate found in the general population. The gap is especially stark for substance use disorders, PTSD, and serious conditions such as schizophrenia. These disparities underscore why social workers in homeless services need specialized training in trauma-informed care, co-occurring disorder treatment, and crisis intervention.
Who Is Most at Risk? Demographics and Disparities
Black Americans made up roughly 12% of the U.S. general population in 2024 yet accounted for 32% of all people experiencing homelessness, according to the HUD Annual Homelessness Assessment Report (AHAR).1 That disparity, visible in 93% of the Continuums of Care (CoCs) tracked by HUD, reflects generations of structural inequities in housing, employment, and access to behavioral health care.2 Understanding who faces the highest risk is essential for social workers designing outreach strategies that actually reach the people who need them.
Racial and Ethnic Disparities
The 2024 AHAR counted approximately 771,480 people experiencing homelessness on a single night.1 White individuals were underrepresented relative to their share of the general population in 93% of CoCs, while Black individuals were overrepresented at roughly the same rate.2 Indigenous, Native Hawaiian, and Pacific Islander populations also face disproportionate risk, although smaller sample sizes make point-in-time estimates less precise. The National Alliance to End Homelessness notes that these gaps persist even when income is controlled for, pointing to discriminatory housing policies, lending practices, and criminal legal system involvement as key drivers.2
Youth Homelessness and Mental Health
About 150,000 children were counted among the homeless population in 2024, representing roughly 20% of the total.1 Research from Chapin Hall's Voices of Youth Count initiative has consistently found that unaccompanied youth experiencing homelessness face elevated rates of depression, post-traumatic stress disorder, and suicidality compared to housed peers. LGBTQ+ youth are overrepresented in this group, often after family rejection. For social workers, the takeaway is clear: mental health resources for homeless youth must be trauma-informed, developmentally appropriate, and culturally responsive from the first point of contact.
Gender Differences in Mental Health Presentations
Men and women experiencing homelessness tend to present with different constellations of mental health challenges. Women report higher rates of PTSD and histories of intimate partner violence, which frequently precipitate episodes of homelessness. Men, on the other hand, report higher rates of substance use disorders. These patterns have practical implications: shelters and outreach programs that use a single-track intake process may miss critical needs. Gender-responsive screening tools help social workers identify the right combination of housing, safety planning, and clinical referrals.
Sheltered vs. Unsheltered Populations
Of the total homeless population counted in 2024, roughly 152,585 people were classified as chronically homeless, representing about 30% of the total.1 A significant share of chronically homeless individuals live unsheltered, sleeping outdoors, in vehicles, or in locations not meant for habitation. This unsheltered group tends to experience more severe mental illness and lower engagement with services than those in emergency shelters or transitional housing. Street outreach teams staffed by social workers play a critical role in building trust over repeated contacts, often over months or years, before individuals are willing to accept help.
Rural vs. Urban Disparities
Homelessness in rural areas is notoriously difficult to count because it often takes the form of doubling up with family, staying in motels, or living in substandard housing rather than appearing in shelters or on the streets. Federal point-in-time counts tend to undercount rural populations for this reason. Compounding the problem, rural communities have far fewer mental health providers per capita, longer travel distances to clinics, and limited public transportation. Social workers practicing in rural settings frequently fill multiple roles, serving as case manager, crisis counselor, and benefits navigator simultaneously. Telehealth social work has expanded access somewhat, but connectivity gaps and digital literacy barriers remain real obstacles.
These disparities are not abstract statistics. They shape who walks through the door of a shelter, who never reaches a shelter at all, and what combination of services will make stable housing achievable. Social workers who understand these demographic and geographic fault lines are better positioned to advocate for equitable funding, design culturally grounded interventions, and push for policy changes that address root causes rather than symptoms.
Black Americans make up roughly 13% of the U.S. population, yet they represent 37 to 40 percent of those experiencing homelessness. This disparity is a direct consequence of systemic inequities, including redlining, unequal access to mental health services, and economic marginalization, not individual behavior. Recognizing homelessness as a structural issue is essential for effective social work intervention.
How Social Workers Help People Experiencing Homelessness
Social workers are the connective tissue between people sleeping on the street and the systems built to house, treat, and stabilize them. The work is hands-on, mobile, and rarely confined to an office. It blends clinical skill with logistical hustle, and it demands a practitioner who can hold a crisis assessment in one hand and a Medicaid application in the other.
Core Roles on the Job
Most social workers in this field rotate through a predictable set of responsibilities, often within the same week:
- Street outreach: Meeting clients in encampments, under bridges, in shelters, and at drop-in centers. Building rapport before pushing any intervention.
- Intake assessment: Screening for mental illness, substance use, medical conditions, domestic violence history, and chronic homelessness status to determine program eligibility.
- Case management: Holding a caseload of 15 to 40 clients, tracking appointments, court dates, treatment plans, and housing applications.
- Crisis intervention: Responding to psychiatric emergencies, overdoses, and acute safety threats, often coordinating with mobile crisis teams or co-responder programs.
- Housing advocacy: Pushing landlords, housing authorities, and continuum-of-care coordinators to move clients up waitlists and into permanent supportive housing.
Trauma-Informed Care as the Default
Effective practitioners assume every client has experienced significant trauma, because most have. That assumption shapes everything: tone of voice, pacing of questions, how choices are offered, and how setbacks are interpreted. Motivational interviewing and harm reduction sit at the center of this approach. Rather than demanding behavior change as a precondition for help, social workers meet clients where they are, reduce immediate risk (clean needles, naloxone, safer-use education), and let stability build the conditions for deeper change.
Integrated Treatment and Systems Navigation
Co-occurring mental illness and substance use disorders are the rule, not the exception, in this population. Modern practice treats them simultaneously through integrated dual diagnosis treatment, not sequentially. A social worker might coordinate a psychiatric medication evaluation, a methadone or buprenorphine induction, and a housing voucher application in the same week for the same client. These responsibilities span micro, mezzo, and macro social work levels, from direct clinical contact to systemic advocacy.
Systems navigation is its own skill set: securing replacement birth certificates and state IDs, applying for Medicaid and SNAP, filing SSI/SSDI claims (often with multiple appeals), and pairing clients with Housing Choice Vouchers, rapid rehousing, or permanent supportive housing slots.
The Cost to the Worker
This field carries a high rate of burnout and secondary traumatic stress. Witnessing repeated client deaths, navigating chronically underfunded systems, and absorbing daily exposure to suffering takes a measurable toll. Strong supervision, peer support, manageable caseloads, and protected time off are not perks in this work. They are clinical infrastructure. Anyone exploring broader careers in social work should understand that homeless services demand both exceptional resilience and robust organizational support.
Related Articles
Evidence-Based Interventions: Housing First, Treatment First, and Beyond
Social workers addressing homelessness rely on two dominant intervention frameworks: Housing First and Treatment First. Understanding how each model works, and where the evidence points, is essential for practitioners choosing the right approach for their clients.
Housing First places individuals directly into permanent housing with no preconditions such as sobriety or treatment compliance. Supportive services are offered but never mandated. Treatment First, by contrast, requires participants to complete psychiatric treatment or substance use programming before they can access permanent housing. The logic is that clinical stability should precede independent living.
The research strongly favors Housing First for housing retention. Studies consistently show that Housing First programs retain 70 to 90 percent of participants in stable housing, compared to just 30 to 60 percent for Treatment First approaches.1 Critically, psychiatric symptom outcomes are similar across both models, and neither approach worsens substance use.1 Quality of life shows modest improvement under Housing First, while Treatment First programs produce no significant improvement on this measure.1
Cost-effectiveness further supports Housing First. Research on VA homeless veterans found that Housing First voucher programs averaged approximately $18,931 per participant, generating meaningful savings relative to emergency shelter cycling and repeated hospitalization.2
Despite this evidence, neither model is a silver bullet. Practitioners working at macro social work levels advocate integrating elements of both, tailoring interventions to individual needs. Some clients benefit from structured treatment environments before transitioning to independent housing, while others thrive when housing stability comes first. Social workers specializing in co-occurring disorders, including those pursuing trauma certifications for social workers, are especially well positioned to navigate these clinical decisions.
The broader takeaway for the field is clear: housing is healthcare. Effective intervention begins with meeting people where they are, both literally and clinically, and building support systems around stable shelter rather than the other way around.
Social Support and Housing Transitions: Why Relationships Matter
The transition from homelessness into stable housing rarely succeeds on a foundation of shelter alone. Social support functions as a critical protective factor that directly influences how long a person remains housed. Research consistently shows that individuals with strong personal networks are significantly less likely to return to homelessness after a housing placement.1
The Protective Power of Relationships
When social workers talk about support networks, they are not referring to a single type of help. Emotional support reduces the isolation and stress that can destabilize a tenancy. Informational support helps people navigate complex systems, from understanding a lease to applying for benefits. Instrumental support provides the tangible assistance that makes daily life possible: transportation to appointments, help moving furniture, or a meal during a crisis, a need that intersects with social work and food insecurity. Each type operates differently, but together they form a buffer against the setbacks that often precede housing loss.2
Research on reentry populations illustrates this vividly. Formerly incarcerated individuals frequently rely on family and friends as their primary housing source for up to a year after release, and the durability of that housing depends heavily on the quality of those relationships.3 The same pattern holds across broader homeless populations. Clients who maintain even one consistent, trusted connection are better equipped to weather the challenges of independent living.
How Social Workers Assess and Build Connections
Effective practice begins with a deliberate assessment of a client's existing network. This goes beyond a simple contact list. Social workers use ecological systems theory in social work to map who provides what kind of support, whether those relationships are healthy or strained, and where gaps exist. For many clients, years of instability have frayed family ties, and rebuilding those bridges requires careful, client-led mediation. In other cases, the available network is strong but overwhelmed, and the social worker's role shifts to shoring up that support with professional resources rather than replacing it.
Peer support merits particular attention because it offers something professional services often cannot: the credibility of shared experience. Peer support groups create spaces where people can exchange practical survival knowledge and feel understood without needing to explain the context of their lives. Studies identify peer connections as a key factor in successful reintegration after homelessness3, and many permanent supportive housing programs now intentionally build peer mentorship into their service models.
Practical Strategies for Permanent Supportive Housing
Social workers can embed relationship-building directly into housing transition plans through several concrete approaches. Building community ties starts early, connecting clients to neighborhood groups, faith communities, or recreational programs before the move-in date so that some familiar faces exist from day one. These attachments to place, where a person feels known and accepted in their immediate environment, are strongly associated with tenancy security and longer housing stays.4
Family reunification, when safe and desired by the client, is another high-impact strategy. This work often involves ongoing mediation, communication skill-building, and gradual reconnection rather than a single reconciliation event. The goal is not just to restore a relationship but to ensure it functions as a reliable source of support rather than a trigger for instability.
Ultimately, the most effective housing interventions treat social connection not as a bonus outcome but as a core component of the support plan. A lease provides the structure. Relationships provide the staying power.
Questions to Ask Yourself
Barriers to Mental Health Services for People Experiencing Homelessness
Approximately 70% of uninsured people experiencing homelessness who are eligible for Medicaid face barriers that prevent successful enrollment, leaving a critical gap in mental health access.1 Nationally, one in five homeless individuals lacks any health coverage, and while 72% are enrolled in Medicaid, the path to that coverage is often blocked by administrative hurdles.2 Without insurance, mental health services become prohibitively expensive or completely out of reach.
Insurance Gaps and Enrollment Obstacles
Medicaid stands as the primary health coverage source for people experiencing homelessness, yet millions encounter systemic barriers during enrollment. Applicants frequently lack a permanent address, a government-issued ID, or the documentation required to prove income and citizenship. Application forms can run dozens of pages, and without a caseworker or navigator, the process is overwhelming. Research published in PubMed Central found that a large share of uninsured homeless adults, more than two-thirds, remain eligible but unenrolled.2 State-level decisions matter too: in nonexpansion states, many adults fall into the coverage gap where they earn too little for marketplace subsidies but too much for traditional Medicaid, leaving mental health treatment financially inaccessible.3
Provider Shortages and Geographic Mismatch
The Health Resources and Services Administration designates thousands of regions across the U.S. as mental health professional shortage areas, and these designations frequently overlap with communities where homelessness is concentrated. Even in urban centers where clinicians are relatively abundant, behavioral health programs serving homeless populations are chronically underfunded and often located far from shelters or encampments. Rural homelessness adds another layer: mobile outreach is scarce, and the nearest psychiatrist may be hours away. This geographic mismatch means that a person ready to seek help for depression or trauma cannot find a provider who will see them in a timely manner, or at all.
Stigma That Blocks Treatment Access
Stigma operates from two directions to discourage mental health care. Internalized shame can lead individuals to feel undeserving of help or to fear being labeled as "crazy" or dangerous. This self-censure delays treatment and deepens isolation. On the provider side, bias often manifests when clinicians treat homeless patients as noncompliant or "difficult," offering shorter appointments and less collaborative care. Research shows that these negative encounters erode trust and reduce the likelihood that a person will return for follow-up. Even when services exist, a hostile or dismissive encounter can turn someone away for months.
Fragmented Systems That Complicate Care
Housing authorities, mental health clinics, substance use treatment programs, and the criminal justice system operate in silos, rarely sharing information or coordinating care. A person discharged from jail may receive no connection to outpatient therapy; those interested in forensic social work can see how professionals bridge this gap. Someone entering a shelter might be required to separately apply for psychiatric services, addiction counseling, and housing assistance, each with its own intake, waitlist, and eligibility rules. Without a single point of coordination, navigating these fractured bureaucracies becomes a full-time burden that many cannot manage alongside the daily struggle for survival. Addressing these barriers demands integrated, low-barrier models that bring services directly to where people are, a principle social workers champion in both clinical social work and macro practice.
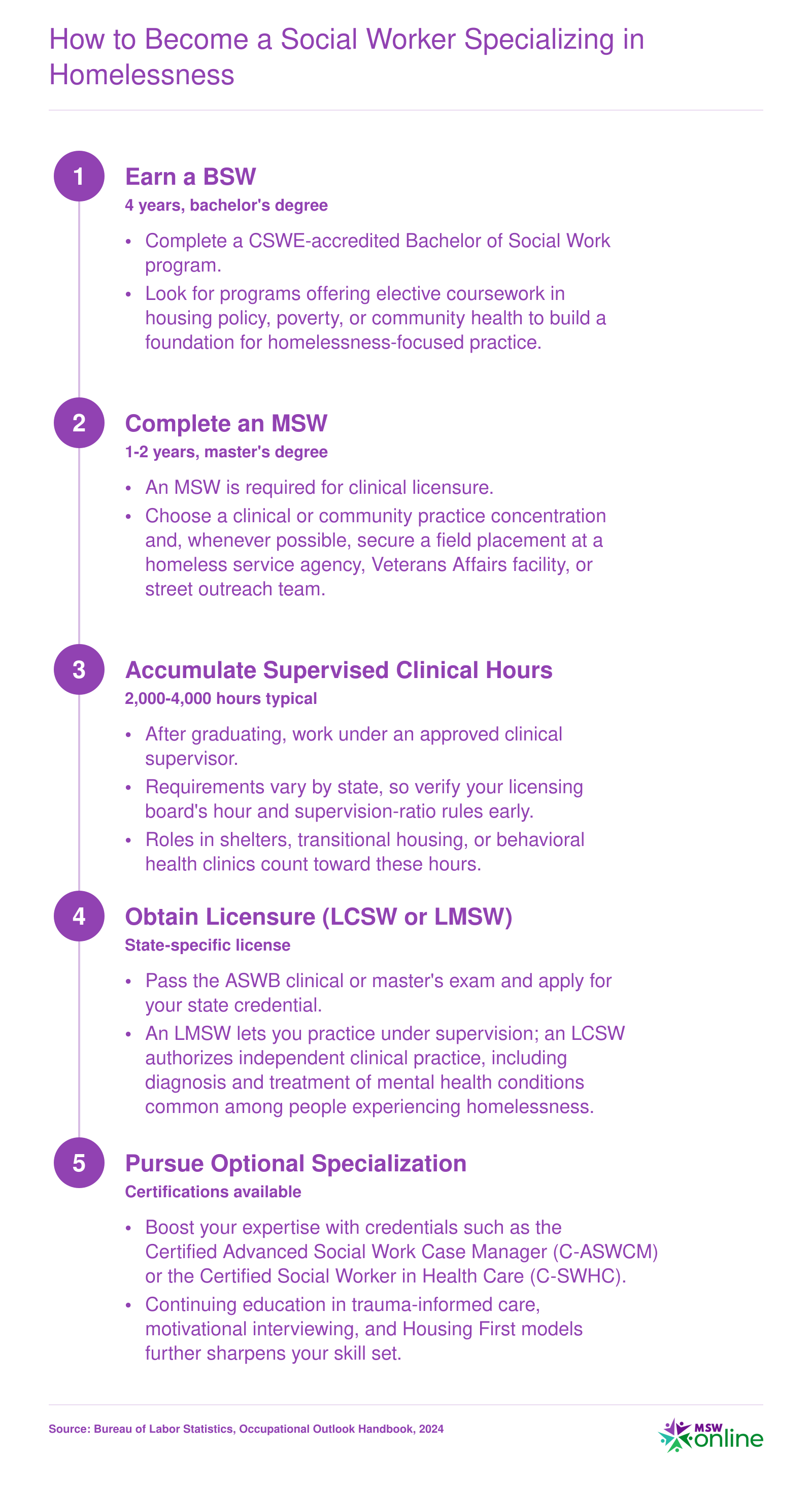
How to Become a Social Worker Specializing in Homelessness
Breaking into homelessness-focused social work follows the same credentialing ladder as other clinical specializations, but intentional practicum placements and targeted certifications set you apart. Field placements at shelters, street outreach programs, or Housing First agencies give you direct exposure to the populations you will serve and strengthen your competitiveness for post-licensure roles. The Bureau of Labor Statistics projects 6% job growth for social workers overall from 2024 to 2034, with even faster growth (roughly 11%) projected for mental health and substance abuse social workers.
Salary and Job Outlook for Social Workers in Homelessness Services
Social workers serving people experiencing homelessness typically fall under several Bureau of Labor Statistics (BLS) occupational categories. The table below shows national median and mean annual wages for the most relevant classifications. Keep in mind that actual compensation varies by employer type (nonprofit, government, healthcare system), geographic region, and years of experience. Social workers in homelessness services frequently hold titles that align with the mental health and substance abuse social worker or child, family, and school social worker categories, depending on their population focus and clinical responsibilities.
| BLS Occupational Title | National Employment | 25th Percentile Wage | National Median Wage | National Mean Wage | 75th Percentile Wage |
|---|---|---|---|---|---|
| Social Workers (broad category) | 759,740 | $48,680 | $61,330 | $67,050 | $78,500 |
| Mental Health and Substance Abuse Social Workers | 125,910 | $46,550 | $60,060 | $68,290 | $78,980 |
| Child, Family, and School Social Workers | 382,960 | $47,480 | $58,570 | $62,920 | $74,060 |
| Healthcare Social Workers | 185,940 | $55,360 | $68,090 | $72,030 | $83,410 |
| Counselors, Social Workers, and Other Community and Social Service Specialists | 2,477,920 | $45,750 | $57,480 | $62,980 | $75,090 |
Frequently Asked Questions About Mental Health and Homelessness
The intersection of mental health and homelessness raises important questions for social workers, students, and anyone working toward solutions. Below are answers to the most common questions, grounded in current research and practice evidence.
Resources for Social Workers and People Experiencing Homelessness
Connecting to the right resources can mean the difference between a crisis that escalates and one that finds a path toward stability. What follows is a curated set of organizations, helplines, and practitioner toolkits that bridge the gap between homelessness and mental health care.
Crisis Helplines and Immediate Support
- 988 Suicide & Crisis Lifeline: Free, confidential phone, text, and chat support for anyone in emotional distress or suicidal crisis. Available 24/7 across the United States. Serves individuals in crisis directly and can be used by social workers to stabilize a client in the moment.
- SAMHSA National Helpline (1-800-662-HELP): A 24/7, free, confidential treatment referral and information service for mental and substance use disorders. Provides referrals to local treatment facilities, support groups, and community-based organizations. This line serves both people experiencing homelessness who are seeking care, and practitioners looking for resources for their clients.
- 211: A universal, three-digit dialing code that connects callers to local community services, including emergency housing, food programs, mental health care, and employment assistance. Social workers can use 211 as a real-time referral shortcut, and individuals can navigate their own local options without needing an appointment.
National Advocacy and Policy Organizations
- National Alliance to End Homelessness (NAEH): A research and policy organization that provides data, toolkits, and advocacy guidance on preventing and ending homelessness. Its resources are geared toward practitioners, agency leaders, and policymakers who need evidence to shape programs.
- NAMI (National Alliance on Mental Illness): A grassroots advocacy group offering peer-led support groups, a national helpline (1-800-950-NAMI), and educational programming for individuals and families affected by mental illness. Local NAMI affiliates often partner with shelters and outreach teams, making them a bridge between clinical care and community support.
- HUD Exchange: A practitioner-facing website housing federal guidance, training materials, and data tools for the Continuum of Care (CoC) system and other HUD homelessness assistance programs. Social workers coordinating entry or applying for grants will find the latest policy updates and technical assistance here.
Practitioner Toolkits and Training
- SAMHSA's TIP Series on Homelessness: The Treatment Improvement Protocol (TIP) collection includes evidence-based guides for clinicians working with people experiencing homelessness, covering engagement strategies, trauma-informed care, and co-occurring disorders. These are free downloads aimed at front-line practitioners.
- HUD's Coordinated Entry Resources: A suite of training modules, assessment tools, and implementation guides that help jurisdictions design or improve coordinated entry systems. Social workers involved in housing placement or case management can use these to standardize prioritization and improve fairness.
- NASW Continuing Education on Trauma-Informed Care: Online courses through the National Association of Social Workers offer CE credits on trauma-informed approaches tailored to homelessness, crisis intervention, and ethical practice with vulnerable populations. Designed for licensed social workers seeking professional development.
Practitioners who want to deepen their clinical expertise in this area may also consider pursuing a psychiatric social worker career path, which focuses specifically on mental health assessment, diagnosis, and intervention for vulnerable populations.
Explore More
- Bilingual Social Worker
- Continuing Education for Social Workers
- COVID-19 Guide for Social Workers
- CSWE Accreditation
- DSW vs. PhD in Social Work
- Environmental Social Work
- Free Implicit Bias Tests & Training Resources
- How Long Does It Take to Become a Social Worker?
- How Social Work Reduces Healthcare Costs
- How to Find a Social Work Job
- Levels of Social Work Licensure
- LGBTQIAP in Social Work
- Micro, Mezzo & Macro Social Work
- MSW Admission Requirements
- MSW Scholarships
- MSW Specializations
- MSW vs. MSSW
- Remote Resources for Mental Health Workers
- Social Work & Food Insecurity
- Social Work & Gun Violence Prevention
- Social Work Ethics
- Social Work Field Placement Guide
- Social Work Grants
- Social Work Internships
- Social Work Theories & Practice Models
- Social Work Volunteer Opportunities
- Social Work vs. Counseling
- Social Work vs. Psychology
- Social Work vs. Sociology
- Social Worker Salary Guide
- Social Worker vs. Therapist
- Social Worker's Guide to Cyberbullying
- Student Mental Health & Social Work on College Campuses
- What Can You Do With an MSW Degree? Careers & Salaries
- Why Is Research Important in Social Work? A Complete Guide
- Women in Social Work Leadership